Therapy Progress Notes: A Step-by-Step Nursing Guide to Writing Progress Notes, Psychotherapy Notes, and Using Therapy Note Templates
Therapy progress notes play an essential role in modern clinical practice, serving as a structured record of a patient’s experiences, responses, and needs across the course of care. Within nursing education, understanding how these notes function—and how they are written—provides students with a foundation for accurate, ethical, and consistent communication in behavioral health and counseling environments. As mental health services continue to evolve, clear and organized documentation remains central to quality care, interdisciplinary collaboration, and continuity across different providers and settings.
Much like how nursing assessments offer a systematic way to evaluate a patient’s physical status, therapy progress notes provide a framework for capturing psychological, emotional, and behavioral changes over time. They are not simply administrative requirements; they are clinical tools that guide decision-making, support coordinated care, and help ensure that treatment remains aligned with patient needs and established standards. Effective documentation also strengthens communication between care teams, supports clinical reasoning, and enhances patient safety by providing a reliable record of observations, concerns, and clinical decisions.
For nursing students, learning how to read, interpret, and write these notes builds confidence in mental health settings and deepens understanding of therapeutic interactions. With growing emphasis on integrated care models, nurses are increasingly expected to participate in documentation that reflects both medical and psychosocial dimensions of health. This requires clarity, precision, and a solid grasp of the foundational concepts that shape professional note-writing across clinical disciplines.
This guide introduces the core principles that underpin therapy progress notes, including their purpose, structure, and use in clinical environments. It explores widely used documentation frameworks, describes how to capture essential behavioral and psychological information, and outlines step-by-step methods for translating observations into clear written records. Through practical explanations, evidence-based strategies, and educational examples, nursing students will gain the knowledge needed to navigate documentation expectations with confidence and competence.
By understanding the role these notes play in patient care and professional accountability, students can strengthen their clinical judgment, communicate more effectively within care teams, and contribute to high-quality, patient-centered mental health practice.
Understanding Therapy Progress Notes
What Are Therapy Progress Notes in Mental Health Documentation?
Therapy progress notes are the clinical records clinicians use to document each encounter with a client. They serve as the primary repository of information about a client’s mental health status over time, capturing the client’s report, observable behavior and mental status, therapeutic interventions used during the session, the clinician’s assessment, and the agreed plan for ongoing care . Unlike privileged psychotherapy process notes—usually kept separate and more reflective of session process—progress notes are part of the treatment record that other members of the care team, auditors, and, in many cases, the client (or insurer) can access under the law. Clear progress documentation therefore balances clinical detail with professional language and legal appropriateness.
Key functions of these notes include:
- Clinical continuity: letting the next clinician quickly understand prior interventions and client response.
- Care coordination: communicating treatment goals and interventions for interdisciplinary teams (nurse, prescriber, social worker).
- Quality, billing, and compliance: demonstrating medical necessity, tracking progress toward treatment goals, and supporting reimbursement audits.
- Risk management and legal record: creating an auditable chain of clinical reasoning should questions arise.
Why Are Progress Notes Important in Nursing and Clinical Care?
Progress notes play a vital role in nursing and mental health care. They allow nurses and mental health professionals to document a client’s responses to interventions, track changes in mental status, and assess whether treatment goals are being met. By recording client care in a structured way, progress notes also help ensure that interventions are tailored to the client’s needs and that therapeutic approaches are documented consistently.
In addition to supporting clinical decisions, therapy progress notes provide a legal and professional record of care. Clear, accurate notes can protect both the client and the clinician by demonstrating that appropriate interventions were used and that the client received standard-of-care treatment. For nursing students, learning to write effective therapy progress notes fosters professionalism and enhances communication within multidisciplinary teams.
What Should Be Included in a Therapy Note or Progress Note?
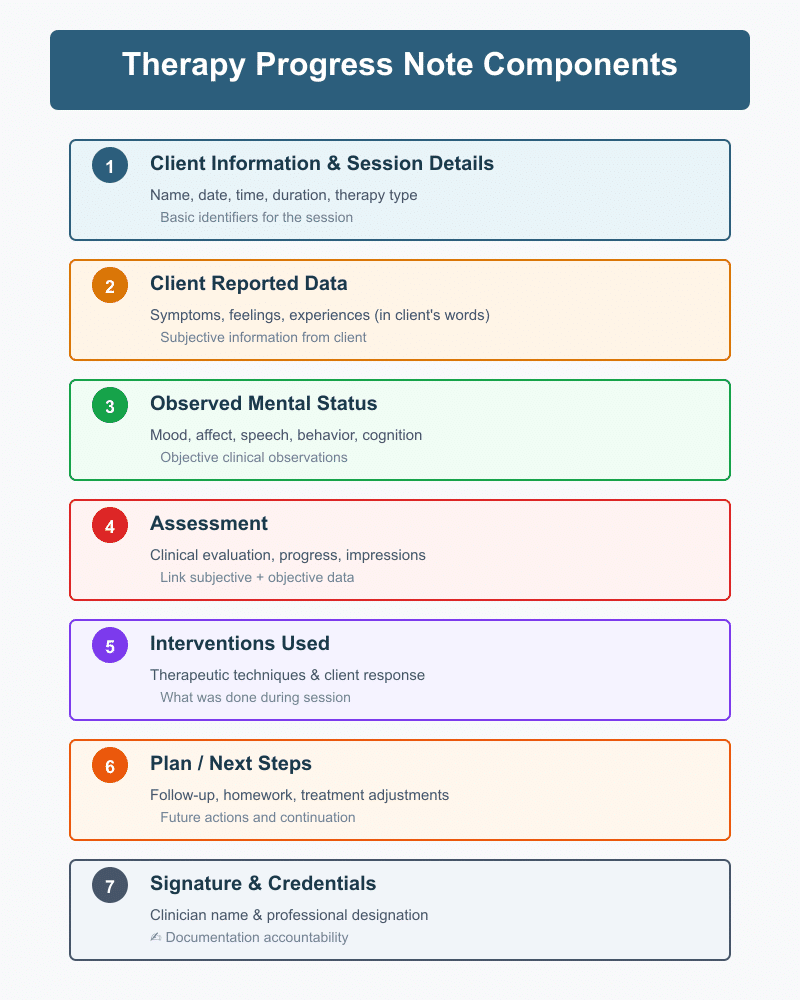
A high-quality therapy note or progress note typically includes several essential components:
- Client Information and Session Details: Include the client’s name, date, time, duration, and type of therapy session.
- Client Reported Data: Summarize the client’s statements about symptoms, feelings, or experiences during the session. Using the client’s own words can enhance clarity.
- Observed Mental Status: Record objective observations such as mood, affect, speech, behavior, and cognitive status. This helps track changes over time.
- Assessment: Provide the clinician’s evaluation of the client’s condition, linking subjective and objective data. Include progress toward treatment goals and clinical impressions.
- Interventions Used: Detail the therapeutic techniques or approaches employed during the session, including the client’s response.
- Plan / Next Steps: Outline follow-up plans, homework, adjustments to the treatment plan, referrals, or continued interventions.
- Signature and Credentials: Indicate who documented the session and their professional designation.
Key Components of Clinical Notes and Mental Health Progress Notes
Writing mental health progress notes involves integrating multiple components into a clear, concise document that captures the client session while reflecting professional standards. The key components include:
- Context and Clinical Purpose: Begin each note by stating the reason for the session and the client’s current concerns. This contextualizes interventions and helps track client progress over time.
- Client Report and Observed Behavior: Clearly differentiate between what the client reported and what the clinician observed. For example, the client may report feeling anxious, while the therapist observes fidgeting or pacing.
- Mental Status Examination: Briefly document relevant elements such as appearance, behavior, mood, affect, speech, thought process, cognition, insight, and judgment. These observations provide objective data to support clinical assessment.
- Interventions and Client Response: Specify which interventions were used during the session, such as cognitive restructuring, grounding exercises, or behavioral activation, and document how the client responded. Linking interventions to outcomes helps track progress toward treatment goals.
- Progress Toward Treatment Goals: Note measurable improvements or setbacks. This could include symptom reduction, increased coping skills, or improvements in functional abilities.
- Plan for Ongoing Care: Conclude with a clear plan, including follow-up sessions, assignments, or referrals. This ensures continuity of care and allows other clinicians to continue tracking client progress effectively.
Sample Therapy Progress Notes
Here are brief examples of how the same session might be documented in different formats:
SOAP Note Example
- S (Subjective): Client reports feeling anxious before an upcoming exam. “I can’t stop worrying and my sleep is poor.”
- O (Objective): Appeared fatigued, slowed speech, alert and oriented ×3.
- A (Assessment): Anxiety related to academic stress; no safety concerns.
- P (Plan): Taught diaphragmatic breathing; assign thought log; follow-up in one week.
DAP Note Example
- D (Data): Client reported increased anxiety and difficulty sleeping; observed pacing and fidgeting.
- A (Assessment): Anxiety impacting functioning and sleep; client demonstrates understanding of coping skills.
- P (Plan): Practice breathing exercises and cognitive restructuring; monitor sleep patterns; review at next session.
BIRP Note Example
- B (Behavior): Client appeared restless and tearful; reported intrusive thoughts about work stress.
- I (Intervention): Psychoeducation on stress management; guided imagery exercise.
- R (Response): Client engaged and reported decreased tension after exercise.
- P (Plan): Continue imagery and relaxation exercises; track stress triggers; follow-up in 1 week.
Understanding SOAP Notes and Other Documentation Formats
Documentation is a cornerstone of mental health care, and nursing students must become proficient in writing clear, accurate, and professional therapy progress notes. Among the most widely used methods, the SOAP note format provides a structured framework for recording clinical encounters. However, alternative formats such as DAP notes and BIRP/PIE notes are also widely used, depending on the therapy session type, client needs, and clinical setting. Understanding these formats ensures that nursing students and mental health professionals can produce high-quality mental health documentation that tracks client progress and supports effective therapy.
What Is the SOAP Note Format and How Is It Structured?
The SOAP note format is a widely recognized note template that organizes session information into four key components:
- S – Subjective: Client-reported experiences, feelings, and concerns during the therapy session.
- O – Objective: Observed behavior, mental status, and measurable data collected by the therapist.
- A – Assessment: Clinician’s interpretation of the client’s mental health status, response to interventions used, and progress toward treatment goals.
- P – Plan: The strategy for ongoing care, including interventions used, homework assignments, adjustments to the treatment plan, and future therapy sessions.
Using a SOAP note template helps nursing students and therapists write therapy notes efficiently while maintaining consistency and clarity. SOAP notes are versatile, supporting documentation for both individual and group therapy sessions, behavioral health interventions, and interdisciplinary communication.
What Does “Subjective” Mean in SOAP Notes During a Therapy Session?
The subjective section is where therapists record client-reported information. This includes descriptions of mood, thoughts, symptoms, or experiences that the client shares during the session. Examples of subjective documentation include:
- “Client reports persistent anxiety and difficulty sleeping for the past three nights.”
- “Client stated, ‘I feel overwhelmed with my responsibilities and unable to cope with stress.’”
Capturing subjective data accurately is critical for mental health progress notes, as it provides context for observed behaviors, informs the assessment, and helps track the client’s progress toward treatment goals over time. Clear subjective entries also support writing effective progress notes by linking client statements to interventions used during therapy.
How to Document Objective Findings and Mental Status Data
The objective section contains clinician observations and measurable data. This includes physical appearance, behavior, speech, affect, cognition, and other elements of the mental status exam. Proper documentation of objective findings strengthens therapy documentation and ensures that progress notes for therapists accurately reflect the session.
Examples of objective documentation:
- “Client appeared tearful, with slowed speech and tense posture.”
- “Mood observed as anxious; affect constricted; oriented ×3; thought process coherent.”
- “Vital signs within normal limits; PHQ-9 score = 12, indicating moderate depressive symptoms.”
Objective findings are essential for tracking client progress, evaluating interventions used, and supporting clinical decision-making in mental health care. Combining subjective and objective data creates a complete picture of the client session, providing a foundation for the assessment and plan.
How to Write Clinical Assessments and Document Interventions Used
The assessment section synthesizes the subjective and objective information into a clinical interpretation. This may include:
- Clinical impressions of the client’s mental health status.
- Progress toward treatment goals.
- Observations about how interventions affected the client during the session.
Documenting interventions used in therapy notes demonstrates active therapeutic engagement and links interventions directly to outcomes. Examples include:
- Guided cognitive restructuring to challenge negative thoughts.
- Psychoeducation on stress management strategies.
- Relaxation or mindfulness exercises to reduce anxiety symptoms.
An effective therapy note should also describe the client’s response to these interventions, for example: “Client practiced diaphragmatic breathing and reported feeling calmer, with anxiety rating reduced from 7/10 to 4/10.”
How to Formulate a Treatment Plan in SOAP Notes
The plan section outlines the next steps in therapy, detailing the interventions used, treatment goals, and follow-up actions. A comprehensive plan in a SOAP note might include:
- Assigning homework or exercises for the client to practice between sessions.
- Adjusting therapy approaches or intensity based on progress.
- Planning the frequency and type of upcoming therapy sessions.
- Coordinating care with other mental health professionals or the interdisciplinary team.
Documenting a clear treatment plan ensures that therapy progress notes remain actionable, allowing therapists and nursing students to track progress and maintain high-quality clinical documentation.
Are There Other Note Formats Besides SOAP for Therapy Documentation?
While SOAP is widely used, nursing students and clinicians should be familiar with other note types, including DAP notes and BIRP/PIE notes, which may better suit certain therapy settings.
DAP Note Format
The DAP note format organizes documentation into Data, Assessment, and Plan. The subjective and objective information are combined in the Data section, streamlining documentation for brief therapy sessions or behavioral health interventions.
Example of a DAP note:
- D (Data): Client reports increased anxiety and restlessness; observed pacing and fidgeting during session.
- A (Assessment): Anxiety interfering with sleep and daily functioning; client shows understanding of coping techniques.
- P (Plan): Continue cognitive-behavioral interventions; assign daily grounding exercises; review at next session.
BIRP/PIE Note Format
The BIRP note (Behavior, Intervention, Response, Plan) emphasizes observed behavior, interventions used, and client response, making it particularly useful in behavioral health and inpatient mental health care. The PIE note (Problem, Intervention, Evaluation) follows a similar approach.
Example of a BIRP note:
- B (Behavior): Client appeared tearful and reported intrusive thoughts.
- I (Intervention): Psychoeducation on coping strategies; guided relaxation exercise.
- R (Response): Client engaged fully and reported decreased tension.
- P (Plan): Continue relaxation exercises; track anxiety triggers; follow-up in one week.
What Is the DAP Note Format and When Is It Used in Psychotherapy?
The DAP note format—standing for Data, Assessment, and Plan—is an alternative to SOAP that is widely used in psychotherapy and behavioral health settings. Unlike SOAP notes, which separate subjective and objective information, the DAP note combines all client-reported and observed data into a single Data section. This makes documentation concise while still capturing essential clinical information.
When is DAP used in psychotherapy?
DAP notes are often used when therapists need a streamlined progress note template to document therapy sessions efficiently. They are particularly common in:
- Behavioral health clinics where multiple clients are seen in a day.
- Outpatient psychotherapy settings where focused session notes are sufficient for tracking progress.
- Cases requiring frequent updates on interventions and client responses without extensive narrative documentation.
Structure of a DAP note:
- Data (D): Combines subjective and objective observations. Document what the client says, how they appear, their mood, behavior, and any relevant mental status findings.
- Example: “Client reported feeling anxious about upcoming exams and observed pacing. Affect constricted, speech slowed.”
- Assessment (A): Clinician interprets the data, noting progress toward treatment goals, responses to interventions used, and clinical impressions.
- Example: “Anxiety levels appear elevated but client demonstrates understanding of grounding techniques and is able to use coping strategies effectively.”
- Plan (P): Outlines the next steps, including therapy interventions, homework, referrals, or adjustments to the treatment plan.
- Example: “Continue cognitive behavioral interventions; assign daily journaling of anxious thoughts; review at next session.”
The DAP format is especially helpful for mental health progress notes that need to be concise yet comprehensive. It allows clinicians to track client progress, record interventions used, and maintain a clear plan for ongoing care.
How Does the BIRP/PIE Format Differ from SOAP Notes?
BIRP and PIE formats are alternative note types that differ from SOAP in focus and organization. Both are often used in behavioral health, inpatient, or intensive therapy settings where detailed documentation of client behavior and response to interventions is critical.
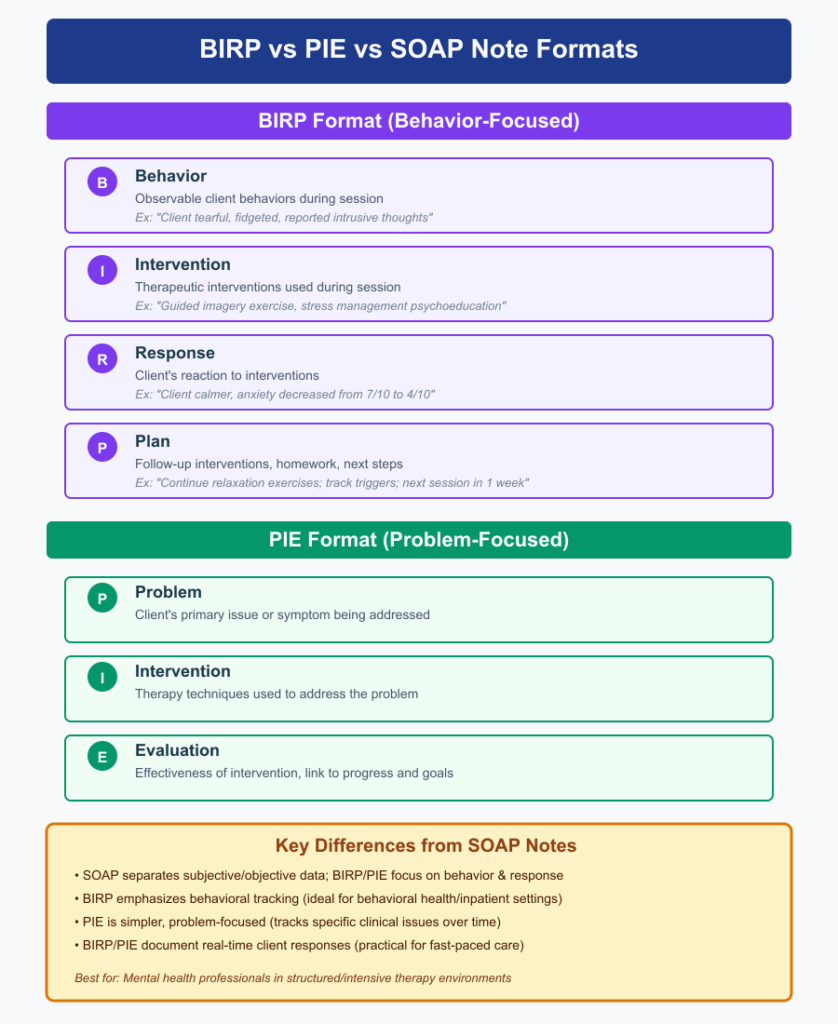
BIRP Note (Behavior, Intervention, Response, Plan):
- Behavior (B): Document observable client behaviors during the therapy session.
- Example: “Client appeared tearful, fidgeted, and reported intrusive thoughts.”
- Intervention (I): Record the therapeutic interventions used during the session.
- Example: “Guided imagery exercise and psychoeducation on stress management provided.”
- Response (R): Note the client’s reaction to the interventions used.
- Example: “Client reported feeling calmer, anxiety rating decreased from 7/10 to 4/10.”
- Plan (P): Detail follow-up interventions, homework, or the next steps in the treatment plan.
- Example: “Continue relaxation exercises; track triggers; next session scheduled in one week.”
PIE Note (Problem, Intervention, Evaluation):
- Problem (P): Identify the client’s primary issue or symptom being addressed.
- Intervention (I): Document therapy techniques or interventions used to address the problem.
- Evaluation (E): Assess the effectiveness of the intervention, linking it to client progress and treatment goals.
Key Differences from SOAP Notes:
- SOAP separates subjective and objective information, while BIRP/PIE focuses more on observed behavior, interventions, and client response.
- BIRP emphasizes behavioral tracking, which is critical for clients in behavioral health or inpatient programs.
- PIE is simpler and more problem-focused, ideal for tracking specific clinical issues over time.
- Both BIRP and PIE allow therapists to document client responses to interventions in real time, making them highly practical for mental health professionals working in fast-paced or structured care environments.
Step-by-Step Guide to Writing Effective Therapy Progress Notes
Writing effective therapy progress notes is an essential skill for nursing students, clinicians, and mental health professionals. Accurate, well-structured notes ensure continuity of care, track client progress, and support high-quality mental health documentation. This step-by-step guide outlines the best practices for creating clear, concise, and actionable therapy notes while incorporating templates and real-world examples.
What Steps Should You Follow to Write Effective Progress Notes?
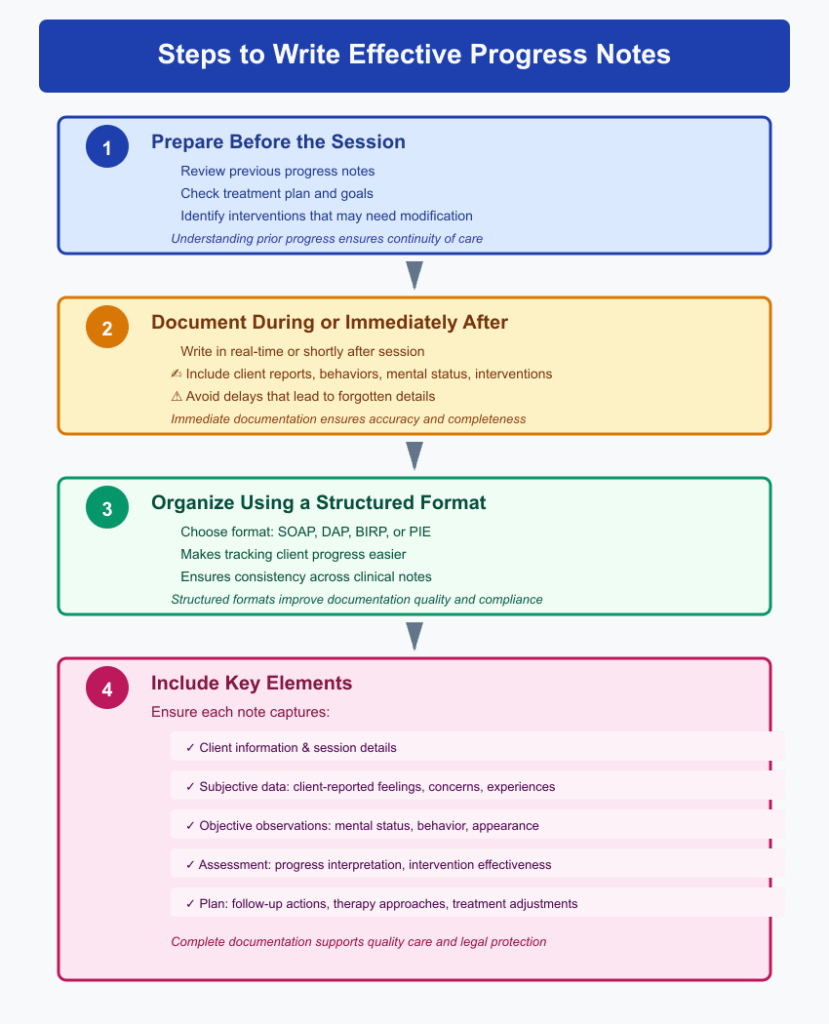
Effective progress notes require a structured approach. Nursing students and clinicians should follow these steps:
- Prepare Before the Session
Review the client’s previous progress notes, treatment plan, and any relevant mental health documentation. This helps you understand progress toward treatment goals and anticipate which interventions used in prior sessions may need modification. - Document During or Immediately After the Session
Writing notes in real-time or shortly after the session ensures accuracy. Include client-reported information, observed behaviors, mental status, and any interventions used. Delaying documentation can result in forgotten details or inaccurate session notes. - Organize Your Note Using a Structured Format
Choose a note format such as SOAP, DAP, or BIRP depending on your setting. Structured formats make it easier to track client progress, ensure all essential elements are documented, and maintain consistency across clinical notes. - Include Key Elements
Ensure that each note captures:- Client information and session details.
- Subjective data: client-reported feelings, concerns, or experiences.
- Objective observations: mental status, behavior, and appearance.
- Assessment: interpretation of client progress, effectiveness of interventions, and current clinical documentation.
- Plan: follow-up actions, therapy approaches, and adjustments to the treatment plan.
How to Gather Relevant Information Before Writing Notes
Gathering comprehensive information before writing therapy notes helps create accurate and meaningful documentation:
- Review Prior Progress Notes: Examine past mental health progress notes to note trends, previous interventions used, and progress toward treatment goals.
- Assess the Client Session: Take detailed observations during the session, focusing on the client’s mental status, behavior, and client reported experiences.
- Include Relevant Health Information: Consider any changes in medications, therapy approaches, or external stressors that may affect the client’s mental health.
- Collaborate with Other Clinicians: Coordinate with interdisciplinary team members when necessary to ensure your notes reflect comprehensive client care.
What Writing Style Works Best for Clinical Notes and Session Notes?
When writing therapy notes or psychotherapy progress notes, clarity, professionalism, and precision are essential:
- Use Clear and Concise Language: Avoid jargon or vague descriptions. Instead of “client seemed off today,” write “Client appeared restless and fidgeted during the session.”
- Be Objective and Specific: Document observable behaviors, specific statements, and measurable outcomes.
- Maintain Professional Tone: Notes should reflect clinical reasoning and therapeutic focus rather than personal opinion.
- Document Interventions and Response: Clearly record which interventions used and how the client responded to them.
Example:
- Effective: “Client practiced cognitive restructuring and reported decreased anxiety from 7/10 to 4/10 after session.”
- Ineffective: “Client seemed better today.”
How to Ensure Clarity and Conciseness When Writing Notes
Clarity and conciseness are critical for maintaining readable and actionable therapy documentation:
- Use Bullet Points or Structured Templates: Break down notes into sections like SOAP, DAP, or BIRP for easy reading.
- Avoid Redundancy: Document only relevant information; skip unrelated details that do not affect client progress or the treatment plan.
- Focus on Outcomes: Highlight progress toward treatment goals and results of interventions used rather than lengthy narrative summaries.
- Use Standard Terminology: Consistent language enhances understanding for other clinicians and protects protected health information.
How to Use Templates to Simplify Therapy Documentation
Using therapy note templates or progress note templates can greatly improve efficiency, especially for nursing students learning to write therapy notes:
- Preformatted Sections: Templates provide placeholders for subjective and objective data, assessments, and plans.
- Consistency Across Sessions: Templates help maintain uniformity in session notes, which is important for tracking client progress over time.
- Time-Saving: Reduces the need to create new notes from scratch, allowing clinicians to focus on therapy delivery.
Example Template Use:
- SOAP note template with sections for client session, mental status, interventions used, and treatment plan.
- DAP template capturing data, assessment, and plan for brief sessions.
- BIRP template for behavioral health tracking.
What Are the Best Therapy Note Templates and Progress Note Examples?
Some commonly used therapy note templates include:
- SOAP Note Template: Sections for subjective data, objective observations, assessment, and plan. Ideal for outpatient or interdisciplinary care.
- DAP Note Template: Combines subjective and objective information into “Data,” followed by assessment and plan. Streamlined for brief therapy sessions.
- BIRP Note Template: Focuses on behavior, interventions used, client response, and plan. Useful for behavioral health, inpatient care, and intensive therapy.
Example of a Progress Note Template in Practice:
Session Date: 18/11/2025
Client: Jane Doe
Therapist: RN Student / Clinician
Session Type: Individual psychotherapy
- S (Subjective): Client reported persistent anxiety before exams; stated, “I feel I can’t cope.”
- O (Objective): Appeared restless, fidgeting; speech slowed; oriented ×3.
- A (Assessment): Anxiety impacting sleep and daily functioning; client demonstrates understanding of grounding techniques.
- P (Plan): Practice diaphragmatic breathing daily; journaling exercises; review at next session.
How to Customize a Note Template for Your Client Session Needs
Every client is unique, so templates should be adapted to meet specific session requirements:
- Include Specific Interventions: Document interventions used tailored to the client’s needs and therapy approaches.
- Track Progress Toward Treatment Goals: Adjust the template to include measurable goals for client progress and response to therapy.
- Add Sections for Special Needs: Include mental status details, behavioral observations, or mental health documentation relevant to the client’s care setting.
- Digital Notes: Use electronic templates to create digital notes, which can be shared securely among clinicians while protecting protected health information.
Customizing templates helps nursing students and clinicians write effective therapy notes, document session outcomes, and maintain comprehensive clinical documentation without sacrificing clarity or detail.
Common Challenges in Writing Progress Notes
Writing therapy progress notes is an essential skill for nursing students and mental health professionals, but it can be challenging. Accurate, clear, and thorough documentation requires attention to detail, critical thinking, and clinical judgment. Understanding common pitfalls and learning strategies to overcome them ensures that session notes, clinical notes, and mental health progress notes remain reliable tools for tracking client progress, guiding interventions used, and supporting effective treatment plans.
What Common Mistakes Do Nursing Students Make in Progress Notes?
Even nursing students with strong clinical knowledge can encounter difficulties when documenting therapy sessions. Some of the most frequent mistakes include:
- Being Too Vague or Subjective
Notes like “Client seemed fine” or “Patient improved” fail to capture specific client information, observed behaviors, or measurable outcomes. Effective therapy notes should clearly document what the client reported, what was observed during the therapy session, and the response to interventions used.- Example of ineffective documentation: “Client appeared anxious.”
- Improved documentation: “Client reported feeling anxious about an upcoming exam, paced the room, and demonstrated shallow breathing; anxiety rated 7/10.”
- Omitting Key Components
Some nursing students forget to include elements such as mental status, interventions used, client progress, or a treatment plan. Missing these details reduces the usefulness of mental health progress notes for future clinical decision-making. - Overloading Notes with Irrelevant Details
Including excessive background information or irrelevant anecdotes can obscure the most important aspects of the session. Effective note writing focuses on information that directly impacts client care and progress tracking. - Using Personal Opinions Instead of Clinical Observations
Writing subjective judgments rather than objective, observable facts compromises the quality of clinical documentation. Notes should be based on measurable outcomes, mental status exam findings, and interventions used, not personal interpretations or assumptions. - Failing to Track Client Progress Over Time
Progress notes should demonstrate movement toward treatment goals. Without longitudinal tracking, therapists cannot determine if therapy approaches are effective or if the client session outcomes are improving.
How to Overcome Writer’s Block When Writing Clinical Documentation
Writer’s block is common, especially for nursing students learning to write therapy notes. Here are strategies to overcome it:
- Use a Structured Note Template
Templates such as SOAP, DAP, BIRP, or progress note templates provide a framework for session notes, guiding the writer to capture all necessary components: subjective data, objective observations, assessment, and plan. - Break the Note into Sections
Focus on one section at a time—document subjective client information, then objective findings, followed by assessment, and finally the treatment plan. This approach reduces overwhelm and ensures thorough documentation. - Document During or Immediately After the Session
Writing therapy progress notes while details are fresh ensures accuracy and minimizes the stress of recalling session information later. - Use Short, Clear Sentences
Concise, professional language helps maintain clarity. Avoid overcomplicating the note with unnecessary narrative. - Leverage Digital Tools or AI Assistants
Many mental health professionals use digital notes or AI assistants to speed up therapy note-taking, organize information, and generate progress note examples for reference while maintaining protected health information standards.
What Should You Do When Unsure What to Document in a Therapy Note?
Uncertainty is common when documenting clinical notes, especially for nursing students. Effective strategies include:
- Focus on Objective and Measurable Data
Document observable behaviors, mental status, and client-reported statements rather than assumptions.- Example: “Client stated, ‘I feel stressed about exams,’ and fidgeted throughout the session” rather than “Client was nervous.”
- Include Interventions and Client Response
Even if unsure about the full clinical interpretation, document the interventions used and the client’s reaction. This allows future therapists or supervisors to evaluate progress toward treatment goals. - Consult Note Templates and Examples
Using therapy note templates or progress note examples provides guidance on standard content, ensuring critical elements such as session notes, assessment, and plan are included. - Ask for Supervision or Feedback
When uncertain, nursing students should seek guidance from a clinician, mental health professional, or supervisor. Reviewing mental health documentation together helps clarify expectations and improve future note writing. - Prioritize Accuracy and Confidentiality
Always document protected health information accurately, even if unsure about interpretation. Avoid guessing or adding unverified information. Document what is observed and reported during the therapy session.
Best Practices for Confidential and Accurate Mental Health Documentation
Maintaining confidential and accurate therapy progress notes is a fundamental responsibility for nursing students, clinicians, and mental health professionals. High-quality mental health documentation supports effective client care, ensures compliance with legal and ethical standards, and provides a clear record of client progress and interventions used. Understanding legal considerations, protecting protected health information, and ensuring accuracy in session notes are essential for safe and professional practice.
What Are the Legal Considerations for Writing Progress Notes?
When writing therapy notes, nursing students and clinicians must follow strict legal guidelines to protect both the client and the healthcare provider. Legal considerations include:
- Compliance with Healthcare Laws and Regulations
- In the United States, the Health Insurance Portability and Accountability Act (HIPAA) requires that mental health progress notes are stored securely, shared only with authorized personnel, and maintained with confidentiality.
- Other regions may have similar laws protecting mental health documentation and client information.
- Accuracy and Completeness
- Incomplete or inaccurate clinical notes can have legal ramifications if documentation is used in audits, insurance claims, or legal proceedings.
- For example, failing to document interventions used or a client’s response during a therapy session could impact liability if a client’s condition worsens.
- Use of Professional Judgment
- Only mental health professionals or supervised nursing students should document therapy notes. Avoid including subjective opinions or unverified information.
- Notes should reflect objective observations, client-reported experiences, mental status, and the outcome of interventions used.
- Timely Documentation
- Delayed progress notes for therapists can be problematic in legal or clinical contexts. Documenting client sessions promptly helps maintain accuracy and protects against potential disputes.
Example: A therapist documenting a cognitive-behavioral session immediately afterward records:
“Client reported anxiety about an exam. Interventions used included diaphragmatic breathing and guided imagery. Client anxiety rating decreased from 8/10 to 5/10. Will continue therapy next session.”
This note is concise, objective, and legally defensible.
How to Ensure Patient Privacy and Protect Mental Health Records
Protecting mental health documentation is essential to uphold ethical standards and client confidentiality. Best practices include:
- Secure Storage of Notes
- Keep therapy notes in locked cabinets or password-protected digital systems.
- Use encrypted electronic health record (EHR) platforms for digital notes.
- Limit Access to Authorized Personnel
- Only individuals involved in the client’s care, such as the therapist, clinician, or supervising nursing staff, should access session notes.
- Avoid sharing client information via unsecured emails or messaging platforms.
- Minimize Identifiable Information
- In shared documentation or case discussions, remove or anonymize client information to protect privacy while still providing useful mental health progress notes.
- Educate Students and Staff
- Nursing students should be trained on mental health documentation, confidentiality policies, and therapy note-taking best practices.
- Regular audits and supervision help ensure compliance with protected health information standards.
Example: Using a therapy note template in an EHR, the clinician can track interventions used, client progress, and treatment goals while keeping identifiable information encrypted and secure.
What Happens When Progress Notes Are Incomplete or Inaccurate?
Incomplete or inaccurate therapy progress notes can have serious consequences for both client care and clinicians:
- Compromised Client Care
- Incomplete documentation may result in missed interventions or miscommunication between clinicians.
- Example: If a therapist fails to record the client’s response to a stress management exercise, the next clinician may repeat ineffective strategies, impacting progress toward treatment goals.
- Legal and Ethical Implications
- Inaccurate notes can be used as evidence in malpractice claims.
- Documentation errors may result in disciplinary action or loss of professional licensure.
- Impact on Treatment Outcomes
- Progress notes for therapists are essential for evaluating the effectiveness of therapy approaches and tracking client progress over time. Missing or inaccurate information hinders therapy planning and mental health care outcomes.
- Professional Reputation and Accountability
- Maintaining accurate session notes, clinical notes, and mental health documentation demonstrates professionalism and commitment to high-quality mental health care.
- Errors can undermine trust with clients and other healthcare team members.
Example: A nursing student documents only “Client was anxious” without specifying severity, behavior, or interventions. The supervising clinician cannot accurately assess client progress or adjust the treatment plan, potentially compromising care and clinical evaluation.
Conclusion
Mastering therapy progress notes is a foundational skill for nursing students and mental health professionals, serving as the backbone of effective clinical documentation and mental health care. Well-written therapy notes not only capture the client’s progress and mental status, but also provide a clear record of interventions used, responses to therapy, and ongoing treatment plans. By understanding structured note formats such as SOAP, DAP, and BIRP, nursing students can ensure that their documentation is consistent, organized, and clinically meaningful.
Accurate session notes and progress note templates help track client progress over time, identify trends in mental health status, and support evidence-based decision-making. At the same time, maintaining confidentiality, protecting protected health information, and adhering to legal and ethical considerations safeguard both the client and the clinician, fostering trust and professionalism.
While challenges like vague documentation, writer’s block, or uncertainty about what to include are common, they can be overcome with structured therapy note templates, careful observation, and guidance from experienced clinicians or mental health professionals. Leveraging best practices in note writing, including clarity, conciseness, and accuracy, ensures that therapy progress notes serve as an effective tool for both therapeutic planning and interdisciplinary collaboration.
Ultimately, mastering the art of writing effective therapy notes empowers nursing students to contribute to high-quality mental health care, track progress toward treatment goals, and deliver effective therapy that is both accountable and client-centered. These skills not only enhance professional competence but also reinforce a commitment to ethical, evidence-based, and high-quality mental health documentation.
Frequently Asked Questions
How to write therapy progress notes?
- Use a Structured Format – SOAP, DAP, or BIRP formats help organize session notes.
- Document Subjective Data – Record what the client reports, including feelings, concerns, or symptoms.
- Include Objective Observations – Note mental status, behavior, appearance, and measurable outcomes.
- Write Assessment – Summarize client progress, response to interventions used, and clinical impressions.
- Plan Next Steps – Outline follow-up actions, therapy adjustments, and treatment plan.
- Be Clear and Concise – Avoid vague statements and use professional, observable language.
How to write progress notes as a nurse?
- Prepare Before Documenting – Review prior progress notes and the patient’s treatment plan.
- Follow a Consistent Format – SOAP or nursing-specific progress note templates ensure completeness.
- Include Relevant Data – Document vital signs, patient-reported symptoms, clinical interventions, and outcomes.
- Track Patient Progress – Highlight changes since the last note and effectiveness of nursing interventions.
- Maintain Confidentiality – Ensure protected health information is secure.
How to write a progress note in simple practice?
- Start with the Date and Patient/Client Info
- Document Observations and Reports – What the client said and what you saw.
- Note Interventions – Actions taken during the session or shift.
- Summarize Progress – Indicate any improvement, setbacks, or continued concerns.
- Plan – Include follow-up or next steps.
Example: “Client reported mild anxiety. Engaged in breathing exercises; anxiety decreased. Continue current interventions and review next session.”
How to Write a Progress Note as a PSW (Personal Support Worker)
- Focus on Daily Care and Observations – Record client mood, behavior, mobility, hygiene, and appetite.
- Use Clear, Objective Language – Avoid opinions; describe what is seen or reported.
- Track Changes – Note any improvements or deterioration in client progress.
- Include Interventions – For example, assisted with mobility, encouraged meals, or facilitated exercises.
- Sign and Date Notes – Maintain accountability and clarity in clinical documentation.
Example: “Client appeared tired but cooperative. Assisted with walking 20 meters. Ate half of lunch. No adverse events. Continue support with mobility and hydration.”