Below is a comprehensive nursing care plan for a patient with ulcerative colitis using the NANDA framework. Ulcerative colitis is a chronic inflammatory bowel disease characterized by inflammation and ulceration of the colon and rectum, often leading to symptoms like diarrhea, abdominal pain, and fatigue. I’ll include multiple nursing diagnoses to address the common issues associated with this condition.
Ulcerative colitis care plans
Nursing Care Plan Ulcerative Colitis Example 1
Nursing Diagnosis 1: Diarrhea
- Statement: Diarrhea related to inflammation of the colon as evidenced by frequent loose, bloody stools (e.g., 6-8 times daily).
- Assessment Data:
- Subjective: Patient reports frequent urgency and loose stools with blood.
- Objective: Stool frequency documented at 7 times in 24 hours, positive for occult blood.
- Expected Outcomes/Goals:
- Patient will have a reduction in stool frequency to 3-4 times daily within 48 hours.
- Patient will report improved control over bowel movements within 72 hours.
- Stool will show no visible blood within 5 days.
- Nursing Interventions:
- Monitor and record stool frequency, consistency, and presence of blood every shift.
- Administer prescribed antidiarrheal medications (e.g., loperamide) or anti-inflammatory drugs (e.g., mesalamine) as ordered.
- Encourage a low-residue diet (e.g., white rice, bananas) to reduce bowel irritation.
- Provide perianal skin care with barrier creams to prevent irritation from frequent stools.
- Educate the patient on hydration importance and encourage oral intake of electrolyte-rich fluids (e.g., oral rehydration solutions).
- Rationale:
- Monitoring stool patterns helps evaluate treatment effectiveness.
- Medications reduce inflammation and slow intestinal motility.
- A low-residue diet minimizes bowel stimulation.
- Skin care prevents breakdown from frequent stools.
- Hydration corrects fluid and electrolyte imbalances caused by diarrhea.
- Evaluation:
- After 48 hours, stool frequency reduced to 4 times daily; goal partially met. No blood visible in stool after 5 days; goal met. Continue monitoring and adjust interventions as needed.
Nursing Diagnosis 2: Acute Pain
- Statement: Acute Pain related to intestinal inflammation and cramping as evidenced by patient reporting abdominal pain at 7/10 and guarding behavior.
- Assessment Data:
- Subjective: Patient describes cramping pain in the lower abdomen.
- Objective: Pain scale 7/10, facial grimacing, and abdominal tenderness on palpation.
- Expected Outcomes/Goals:
- Patient will report pain reduced to 3/10 or lower within 4 hours.
- Patient will demonstrate relaxed posture and reduced guarding within 24 hours.
- Nursing Interventions:
- Assess pain level, location, and characteristics every 4 hours using a pain scale.
- Administer prescribed analgesics (e.g., acetaminophen) or antispasmodics (e.g., hyoscyamine) as ordered.
- Apply a warm compress to the abdomen for 15-20 minutes every 4 hours, if not contraindicated.
- Teach relaxation techniques (e.g., deep breathing or guided imagery) to manage pain perception.
- Position patient comfortably (e.g., knees flexed) to reduce abdominal tension.
- Rationale:
- Pain assessment guides intervention effectiveness.
- Medications target pain and spasms caused by inflammation.
- Heat promotes muscle relaxation and comfort.
- Relaxation techniques reduce stress-induced pain exacerbation.
- Positioning decreases pressure on inflamed areas.
- Evaluation:
- Pain reduced to 2/10 after 4 hours with medication and heat application; goal met. Patient reports improved comfort and relaxed posture; goal met.
Nursing Diagnosis 3: Imbalanced Nutrition: Less Than Body Requirements
- Statement: Imbalanced Nutrition: Less Than Body Requirements related to decreased appetite and malabsorption as evidenced by 5% weight loss in 1 month and reports of nausea.
- Assessment Data:
- Subjective: Patient reports poor appetite and nausea after eating.
- Objective: Weight decreased from 150 lbs to 142 lbs in 4 weeks, BMI dropped from 22 to 21.
- Expected Outcomes/Goals:
- Patient will maintain current weight or gain 1-2 lbs within 2 weeks.
- Patient will tolerate small, frequent meals without nausea within 72 hours.
- Nursing Interventions:
- Weigh patient weekly and monitor trends.
- Collaborate with a dietitian to create a high-calorie, high-protein, low-residue meal plan.
- Offer small, frequent meals (e.g., 5-6 times daily) and nutritional supplements (e.g., Ensure).
- Administer antiemetics (e.g., ondansetron) as prescribed before meals if nausea persists.
- Educate patient on avoiding trigger foods (e.g., spicy or high-fiber items) during flare-ups.
- Rationale:
- Weight monitoring tracks nutritional status.
- A tailored diet meets caloric needs while minimizing irritation.
- Small meals are easier to digest and reduce nausea.
- Antiemetics improve food tolerance.
- Avoiding triggers prevents exacerbation of symptoms.
- Evaluation:
- After 72 hours, patient tolerates 5 small meals daily without nausea; goal met. Weight stable at 142 lbs after 1 week; goal partially met—continue plan and reassess in 1 week.
Nursing Diagnosis 4: Fatigue
- Statement: Fatigue related to chronic inflammation and anemia as evidenced by patient reporting low energy and hemoglobin level of 10 g/dL.
- Assessment Data:
- Subjective: Patient states, “I feel tired all the time and can’t do my usual activities.”
- Objective: Hemoglobin 10 g/dL (normal: 12-15 g/dL for females, 13-17 g/dL for males), pale skin observed.
- Expected Outcomes/Goals:
- Patient will report improved energy levels within 1 week.
- Patient will perform light activities (e.g., walking) without exhaustion within 10 days.
- Nursing Interventions:
- Assess fatigue level daily using a 0-10 scale.
- Monitor lab values (e.g., hemoglobin, iron levels) and report abnormalities to the physician.
- Administer iron supplements or blood transfusions as prescribed for anemia.
- Plan rest periods between activities (e.g., 15-30 minutes every 2 hours).
- Teach energy conservation techniques (e.g., sitting while grooming).
- Rationale:
- Fatigue assessment evaluates progress.
- Lab monitoring identifies anemia severity.
- Supplements/transfusions correct anemia, improving oxygen delivery.
- Rest prevents overexertion.
- Conservation techniques maximize energy use.
- Evaluation:
- After 1 week, patient reports fatigue reduced from 8/10 to 4/10; goal partially met. Patient walks 10 minutes without exhaustion after 10 days; goal met.
Below is a table summarizing the comprehensive nursing care plan for ulcerative colitis based on the NANDA framework. Each nursing diagnosis is organized with its components: diagnosis statement, goals, interventions, rationales, and evaluation. Due to space constraints, I’ve condensed some details, but it captures the essence of the plan.
| Nursing Diagnosis | Expected Outcomes/Goals | Nursing Interventions | Rationale | Evaluation |
|---|---|---|---|---|
| Diarrhea<br>Diarrhea related to inflammation of the colon as evidenced by frequent loose, bloody stools (6-8 times daily). | – Stool frequency reduced to 3-4 times daily within 48 hours.<br>- No visible blood in stool within 5 days.<br>- Improved bowel control within 72 hours. | 1. Monitor stool frequency and characteristics every shift.<br>2. Administer antidiarrheals (e.g., loperamide) as ordered.<br>3. Encourage low-residue diet.<br>4. Provide perianal skin care.<br>5. Educate on hydration with electrolyte fluids. | 1. Tracks treatment effectiveness.<br>2. Reduces motility/inflammation.<br>3. Minimizes bowel irritation.<br>4. Prevents skin breakdown.<br>5. Corrects fluid/electrolyte loss. | After 48 hours, stool frequency 4/day (partially met); no blood after 5 days (met). Continue monitoring. |
| Acute Pain<br>Acute Pain related to intestinal inflammation as evidenced by pain 7/10 and guarding behavior. | – Pain reduced to 3/10 within 4 hours.<br>- Relaxed posture, no guarding within 24 hours. | 1. Assess pain every 4 hours.<br>2. Administer analgesics/antispasmodics as ordered.<br>3. Apply warm compress to abdomen.<br>4. Teach relaxation techniques.<br>5. Position patient comfortably. | 1. Guides intervention efficacy.<br>2. Targets pain/spasms.<br>3. Promotes relaxation.<br>4. Reduces stress-induced pain.<br>5. Decreases abdominal tension. | Pain 2/10 after 4 hours (met); relaxed posture after 24 hours (met). |
| Imbalanced Nutrition: Less Than Body Requirements<br>Imbalanced Nutrition related to decreased appetite and malabsorption as evidenced by 5% weight loss and nausea. | – Maintain/gain 1-2 lbs within 2 weeks.<br>- Tolerate small meals without nausea within 72 hours. | 1. Weigh weekly.<br>2. Collaborate with dietitian for high-calorie, low-residue plan.<br>3. Offer small, frequent meals/supplements.<br>4. Administer antiemetics as prescribed.<br>5. Educate on avoiding trigger foods. | 1. Monitors nutritional status.<br>2. Meets caloric needs safely.<br>3. Improves digestion/tolerance.<br>4. Reduces nausea.<br>5. Prevents symptom flare-ups. | Tolerates 5 meals/day without nausea after 72 hours (met); weight stable at 142 lbs after 1 week (partially met). |
| Fatigue<br>Fatigue related to chronic inflammation and anemia as evidenced by low energy and hemoglobin 10 g/dL. | – Improved energy levels within 1 week.<br>- Perform light activities without exhaustion within 10 days. | 1. Assess fatigue daily (0-10 scale).<br>2. Monitor labs (hemoglobin/iron).<br>3. Administer iron supplements/transfusions as ordered.<br>4. Plan rest periods.<br>5. Teach energy conservation techniques. | 1. Evaluates progress.<br>2. Identifies anemia severity.<br>3. Corrects oxygen delivery.<br>4. Prevents overexertion.<br>5. Maximizes energy use. | Fatigue 4/10 after 1 week (partially met); walks 10 minutes without exhaustion after 10 days (met). |
Notes:
- Assessment Data: Omitted from the table for brevity but included in the original response (e.g., subjective/objective findings like stool frequency, pain scale, weight loss, hemoglobin levels).
- Adjustments: The plan can be tailored based on patient response, such as increasing interventions if goals aren’t met.
- Collaboration: Involves physicians (for medications), dietitians, and other team members as needed.
Summary
This care plan addresses key issues in ulcerative colitis: diarrhea, pain, nutrition, and fatigue. Each diagnosis follows the NANDA structure with a clear problem, etiology, evidence, goals, interventions, rationales, and evaluation. Adjustments can be made based on the patient’s response, disease severity, or additional complications (e.g., dehydration or infection).
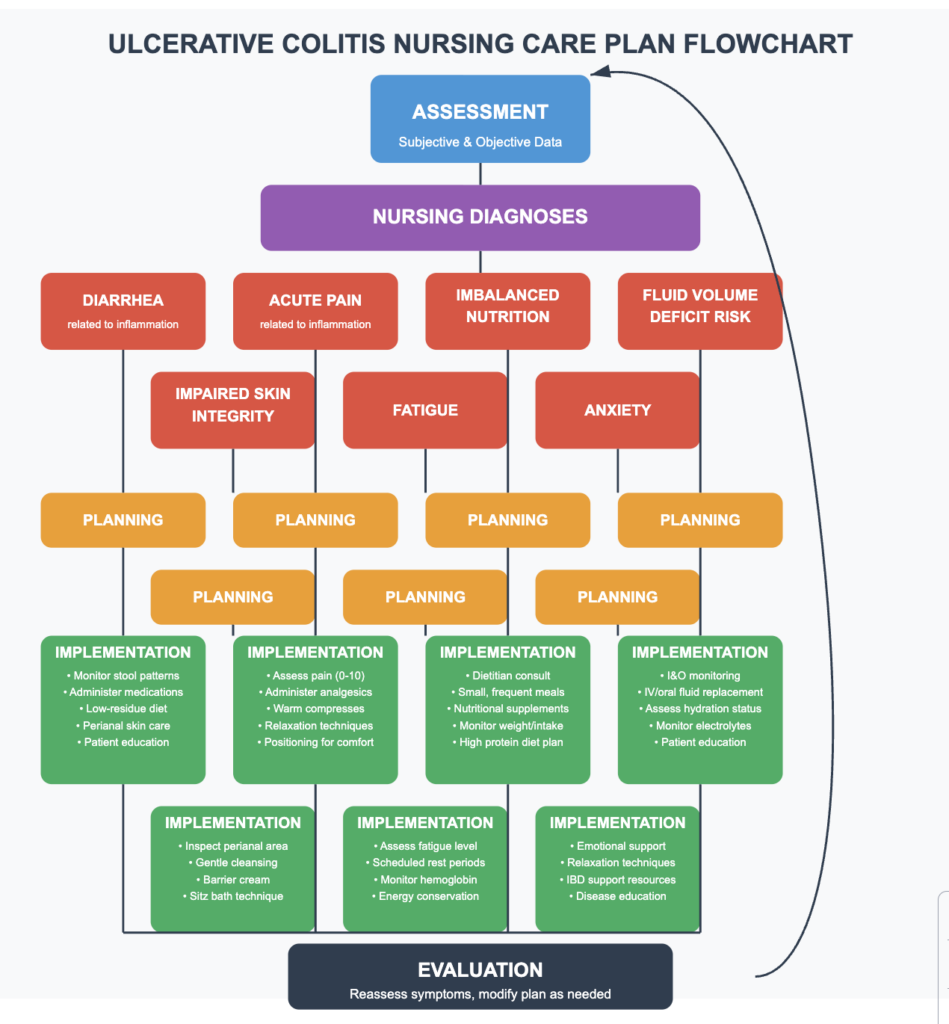
Comprehensive Nursing Care Plan: Ulcerative Colitis
Assessment
Subjective Data:
- Frequent loose, bloody stools (typically 4-8 per day)
- Abdominal pain and cramping, often in lower left quadrant
- Urgency to defecate and tenesmus (painful straining)
- Fatigue and malaise
- Decreased appetite
- Weight loss
- Sleep disturbances related to nocturnal bowel movements
Objective Data:
- Vital signs: Potential tachycardia, low-grade fever
- Weight below baseline
- Laboratory findings: Anemia, elevated inflammatory markers (ESR, CRP), hypoalbuminemia
- Abdominal tenderness on palpation
- Hyperactive bowel sounds
- Pale conjunctiva (if anemic)
- Colonoscopy findings: Continuous inflammation beginning at rectum, extending proximally
Nursing Diagnoses
Diagnosis #1: Diarrhea
Related to: Inflammatory process in colon mucosa As evidenced by: Frequent loose, bloody stools, urgency, and abdominal cramping
Goals/Outcomes:
- Patient will report decreased stool frequency to 2-3 stools/day within one week
- Patient will report formed stool consistency without visible blood within two weeks
- Patient will identify dietary triggers that exacerbate symptoms
Interventions:
- Monitor and document stool characteristics (frequency, consistency, amount, color)
- Administer prescribed medications (anti-inflammatories, immunosuppressants)
- Provide education on a low-residue diet during flares
- Ensure adequate hydration and electrolyte replacement
- Implement a perianal skin care protocol after each bowel movement
- Teach the patient to monitor and record bowel patterns at home
Diagnosis #2: Acute Pain
Related to: Intestinal inflammation and increased motility, As evidenced by: Abdominal cramping, verbal reports of pain, and guarding behavior
Goals/Outcomes:
- Patient will report pain at ≤3/10 within 48 hours
- Patient will demonstrate use of non-pharmacological pain management techniques
- Patient will verbalize understanding of pain management regimen
Interventions:
- Assess pain characteristics using a standardized scale
- Administer prescribed analgesics and antispasmodics
- Apply warm compress to the abdomen as tolerated
- Teach relaxation techniques for pain management
- Position patient for comfort (side-lying with knees flexed)
- Document the effectiveness of interventions
Diagnosis #3: Imbalanced Nutrition: Less Than Body Requirements
Related to: Decreased appetite, malabsorption, and increased metabolic demands, As evidenced by: Weight loss, decreased albumin levels, and inadequate food intake
Goals/Outcomes:
- The patient will consume 75% of meals within 5 days
- The patient will demonstrate no further weight loss during hospitalization
- Patient will verbalize understanding of nutritional needs and dietary modifications
Interventions:
- Consult with a dietitian for a personalized nutrition plan
- Provide small, frequent meals (6 per day)
- Monitor daily caloric intake and weight
- Administer parenteral nutrition if ordered
- Provide nutritional supplements between meals
- Educate on a high-calorie, high-protein, low-residue diet during flares
Diagnosis #4: Risk for Deficient Fluid Volume
Related to: Excessive fluid loss through diarrhea, As evidenced by: Frequent loose stools, potential for dehydration
Goals/Outcomes:
- Patient will maintain balanced fluid status as evidenced by stable vital signs
- Patient will demonstrate adequate hydration (moist mucous membranes, good skin turgor)
- Patient will verbalize understanding of hydration needs
Interventions:
- Monitor intake and output strictly
- Assess for signs of dehydration (dry mucous membranes, poor skin turgor)
- Administer IV fluids as prescribed
- Encourage oral fluid intake of 2-3 liters daily
- Monitor electrolyte levels and replace as needed
- Educate on the importance of fluid replacement during diarrhea episodes
Diagnosis #5: Impaired Skin Integrity (or Risk for)
Related to: Frequent bowel movements and perianal irritation. As evidenced by: Perianal redness, irritation, or breakdown
Goals/Outcomes:
- Patient’s perianal skin will remain intact or show improvement
- Patient will demonstrate proper perianal care techniques
- Patient will verbalize understanding of skin protection measures
Interventions:
- Inspect perianal area with each bowel movement
- Implement gentle cleansing with water (avoid harsh soaps)
- Apply barrier cream or ointment after cleansing
- Teach sitz bath technique
- Use soft, moistened wipes instead of toilet paper
- Provide cotton underwear and loose-fitting clothing
Diagnosis #6: Fatigue
Related to: Inflammatory process, anemia, and sleep disruption As evidenced by: Verbalized exhaustion, decreased activity tolerance
Goals/Outcomes:
- Patient will report improved energy levels within one week
- Patient will balance activity with rest periods
- Patient will verbalize understanding of energy conservation techniques
Interventions:
- Assess fatigue level daily using standardized scale
- Schedule activities during peak energy periods
- Implement planned rest periods
- Monitor hemoglobin levels and administer iron supplements if prescribed
- Provide uninterrupted sleep periods when possible
- Teach energy conservation techniques
Diagnosis #7: Anxiety
Related to: Chronic illness, unpredictable symptoms, and lifestyle adjustments As evidenced by: Expressed concerns, restlessness, or increased questioning
Goals/Outcomes:
- Patient will verbalize decreased anxiety within 3 days
- Patient will identify two effective coping strategies
- Patient will express understanding of disease management
Interventions:
- Provide emotional support and active listening
- Teach relaxation techniques (deep breathing, guided imagery)
- Provide accurate information about ulcerative colitis
- Connect with IBD support resources or groups
- Consider referral to mental health professional if needed
- Encourage expression of fears and concerns
Evaluation
- Reassess symptoms daily and compare to baseline
- Monitor response to medication therapy
- Evaluate nutritional status and weight trends
- Assess patient’s understanding of disease management
- Determine effectiveness of interventions
- Modify care plan as needed based on patient’s response
This comprehensive care plan addresses the major nursing diagnoses commonly encountered when caring for patients with ulcerative colitis and should be individualized based on each patient’s specific presentation and needs.
Related Article: Crohn’s Disease: Nursing Diagnoses, Care Plans, Assessment & Interventions
FAQs Ulcerative Colitis
What are nursing interventions for Crohn’s disease?
Nursing interventions for Crohn’s disease include pain management, nutrition support, medication administration, patient education on disease management, and monitoring for complications such as fistulas or obstructions.
What are the 5 nursing plans?
The five components of a nursing plan are: (1) Assessment, (2) Diagnosis, (3) Planning, (4) Implementation, and (5) Evaluation. These steps guide the nursing process in providing comprehensive care to patients.
What is the nursing role in Crohn’s disease?
The nursing role in Crohn’s disease involves assessing symptoms, administering treatments, providing patient education, offering emotional support, and collaborating with the healthcare team to manage the disease effectively.
What is the treatment plan for Crohn’s disease?
The treatment plan for Crohn’s disease typically includes medications to reduce inflammation and suppress the immune system, dietary modifications, stress management, and in some cases, surgical interventions. The plan is tailored to each patient’s specific needs and disease severity.
In conclusion, nursing care plans for inflammatory bowel disease, including Crohn’s disease and ulcerative colitis, are essential tools for providing comprehensive, patient-centered care. By understanding the nuances of IBD management, implementing effective interventions, and empowering patients through education, nurses play a crucial role in improving outcomes and quality of life for individuals living with these chronic conditions.
 Online | Privacy policy
Online | Privacy policy