Introduction to SBAR Nursing
SBAR is a structured communication framework that can help teams share information about the condition of a patient or team member or about another issue your team needs to address. For nurses working in today’s complex healthcare environments, effective communication is not just a skill—it’s a necessity. The SBAR nursing communication tool has revolutionized how healthcare professionals share critical patient information. As an RN, mastering this structured communication technique can dramatically improve patient outcomes and enhance interprofessional relationships.
What is SBAR in Nursing?
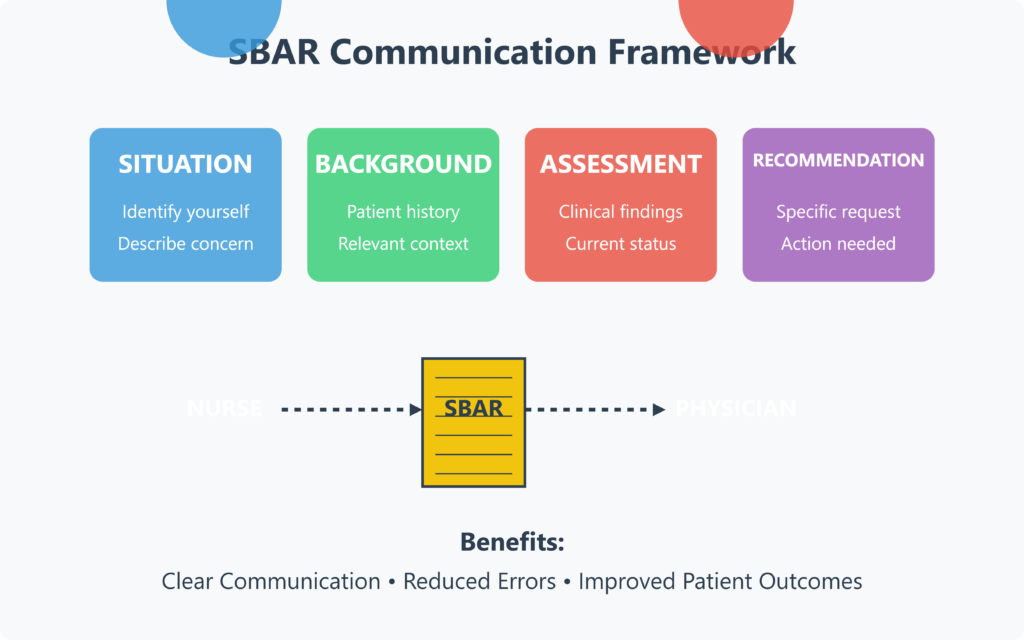
SBAR stands for Situation, Background, Assessment, and Recommendation. This structured communication tool was originally developed by the U.S. Navy for nuclear submarine operations but has since become a cornerstone of nursing practice. SBAR in nursing provides a clear framework for healthcare professionals to communicate vital patient information concisely and effectively.
The SBAR method offers a systematic approach to patient handoff, ensuring that all relevant information is communicated during shift handover or when reporting to physicians. By using the SBAR tool, nurses can organize their thoughts coherently, reducing communication errors that might otherwise compromise patient safety.
Essence of SBAR Nursing Communication
In any healthcare setting, from general medical floors to the intensive care unit, clear communication is essential. A systematic review of communication failures in healthcare revealed that poor handoff communication contributes significantly to adverse patient events. The implementation of the SBAR communication technique has been shown to reduce these incidents substantially.
Nursing students are now taught the SBAR method early in nursing school, emphasizing its importance in developing professional communication skills. Using the SBAR tool consistently throughout a nursing career helps establish good habits that improve patient care and professional relationships.
How to Use the SBAR Method Effectively
| SBAR Component | Purpose | Key Elements | Example |
|---|---|---|---|
| Situation | Identify yourself and briefly describe the current issue | Your name and role Patient name/location Concise problem statement | “This is Nurse Garcia from Med-Surg. I’m calling about Mrs. Smith in room 423, who’s experiencing acute chest pain.” |
| Background | Provide relevant contextual information | Brief admission History Diagnosis Recent relevant events | “She was admitted yesterday with pneumonia. History of MI 2 years ago. Pain started 20 minutes ago.” |
| Assessment | Share your professional evaluation | Vital signs Clinical observations Recent changes Your concerns | “BP elevated at 162/94, pulse 112. Pain is 8/10, radiating to left arm. ECG shows ST elevation.” |
| Recommendation | Clearly state what you need | Specific request Timeframe Questions | “I recommend you come assess her now. Should I call the rapid response team and prepare aspirin?” |
Situation
The first component of SBAR nursing communication involves clearly stating the current situation. When you use SBAR to communicate with other healthcare providers, begin by identifying yourself, your unit, and your patient. Then briefly describe what is happening that prompted your communication.
For example: “This is Sarah, RN from the medical care unit. I’m calling about Mr. Johnson in room 215, who is experiencing sudden shortness of breath and dropping oxygen levels.”
Background
Next, provide concise background information about the patient that relates to the current situation. This helps establish context for the healthcare team.
An SBAR report might continue: “Mr. Johnson is a 67-year-old patient admitted yesterday with pneumonia. He has a history of COPD and was stable on 2L oxygen until about 30 minutes ago.”
Assessment
In this section of the SBAR nursing framework, share your professional assessment of the situation. This is where your clinical communication skills and nursing practice expertise become evident.
“His oxygen saturation has dropped from 95% to 88% despite increasing oxygen to 4L. He’s using accessory muscles to breathe, has a respiratory rate of 28, and is becoming anxious. I suspect his pneumonia may be worsening or he could be developing a pneumothorax.”
Recommendation
Finally, state your recommendation or what you need from the other healthcare professional. Being clear about what you’re requesting helps avoid communication errors.
“I recommend coming to assess him now and possibly ordering a stat chest X-ray. Also, should I prepare for possible intubation equipment?”
SBAR in Nursing Example
Situation
The CDC provides that 12 million Americans have COPD, but more than 12 million others have lung function impairment and may be undiagnosed (CDC, 2020). COPD is the third leading cause of death in the US and affects almost 26 million people. Tobacco use contributes to about 75% of COPD cases. Preventing COPD in the US requires implementing healthcare policies that address risk factors such as smoking.The Family Smoking Prevention and Tobacco Control Act (Tobacco Control Act) was signed into law on June 22, 2009, to protect the American people and create a healthier future. The policy or law gives the FDA authority to regulate tobacco products’ manufacture, distribution, and marketing. The policy led to a $0.62 increase in tobacco products taxation. However, no increase in taxes has occurred since then. If this policy is not enacted adequately, tobacco will continue to contribute to the majority of COPD cases (75%) and associated deaths (40.5 deaths per 100,000 among US men and 34.3 per 100,000 among US women) (CDC, 2020). COPD will continue to be the third contributor to deaths in the US.
Background
Individuals and organizations, including The American Cancer Society Cancer Action Network, BeTobaccoFree.gov, UCSF Center for Tobacco Control Research and Education, National Networks for Tobacco Control and Prevention, American Lung Association, World Lung Foundation, The Legacy Foundation, Americans For Nonsmoker’s Rights have a special interest in the issue. Their primary interest is to reduce tobacco use and minimize the risks of tobacco-related illnesses like COPD and associated death and promote healthier lifestyles. The policymaker is interested in promoting healthier America, and also in protecting tobacco manufacturers, distributors, and retailers, who are also a part of the economy. However, the burden of COPD is more significant, with a cost of about $49 billion annually. Therefore, policymakers should consider the policy and how it can help reduce tobacco use.
As nurses, we are equipped with a responsibility to promote healthier lifestyles. We are also responsible for advocating for health issues like COPD and tobacco use and the patients. Nurses have the necessary skills and knowledge to help patients quit smoking by educating them. Nurses deal with COPD patients every day, and they understand their struggle, including the lack of a cure. Preventative measures become necessary; a reason nurses are advocating for policies to reduce tobacco use. I have had family members and friends who developed COPD, and some have died from its effects in the long run. It is sad to see people die from a disease that can be prevented or minimized in the first place.
Assessment
COPD contributes significantly to mortality rates in the US. Over 6% of the population has been diagnosed with COPD, and nearly the same percentage has lung function impairment and may not be diagnosed (CDC, 2020). This information indicates that the COPD disease burden is greater than reported. As a nurse, I have encountered many patients suffering from COPD, and many have died from its effects. Having a disease as the third contributor to deaths in the country is saddening and shows that relevant stakeholders are not doing enough to enable preventative care.
Many stakeholders are involved in efforts to reduce tobacco use consumption to promote healthier communities and reduce the disease burden. Adequate utilization of the policy to minimize tobacco consumption would help stakeholders like National Networks for Tobacco Control and Prevention, American Lung Association, World Lung Foundation, and policymakers achieve positive results in their efforts. The 2009 law has helped prevent over 350,000 teens from smoking and saved about $31 billion in tobacco use-related costs (Truth Initiative, 2019). This information shows that the policy can be more effective if utilized adequately.
The policy is supported by the American Cancer Society Cancer Action Network, BeTobaccoFree.gov, UCSF Center for Tobacco Control Research and Education, National Networks for Tobacco Control and Prevention, American Lung Association, World Lung Foundation, The Legacy Foundation, Americans for Nonsmoker’s Rights.
Recommendation/Request
The involved organizations and policymakers need to consider implementing an annual tobacco product tax increase at a consistent rate to discourage tobacco use further. The $0.62 tax increase in 2009 had a significant impact. However, people need to feel the impact of tax increases each year to quit or reduce tobacco products consumption. We hope as the healthcare community that the involved stakeholders will consider this proposal with the attention it deserves to save American lives. Thank you for the time and attention you have invested in this matter. As a nurse, I will continue to offer my assistance and expertise based on my knowledge and understanding of the situation to ensure the policy helps promote healthier communities and save lives.
References
American Lung Association (2021). 2021 federal action plan: tobacco priorities. https://www.lung.org/policy-advocacy/federal-action-plan/tobacco-priorities
CDC. (2020). Public health strategic framework for COPD prevention. https://www.cdc.gov/copd/pdfs/framework_for_copd_prevention.pdf
CDC. (2018, February 21). COPD costs. https://www.cdc.gov/copd/infographics/copd-costs.html
Truth Initiative. (2019, June). A decade of the tobacco control act: Where are we now? https://truthinitiative.org/research-resources/tobacco-prevention-efforts/decade-tobacco-control-act-where-are-we-now
SBAR Nursing Template (PDF and Printable)
Hospitals and nursing schools often use SBAR report templates to standardize communication. Below is a general format:
SBAR Report Template
| Section | Details to Include |
| Situation | Patient’s name, current condition, immediate concern |
| Background | Medical history, past treatments, recent changes |
| Assessment | Current vitals, symptoms, nurse’s evaluation |
| Recommendation | Suggested actions, medication adjustments, follow-up plans |
Downloadable SBAR Report Sheet (PDF) Many organizations provide nursing SBAR templates in PDF format for documentation. These templates ensure consistency in reporting.
Benefits of SBAR in Nursing Practice
Research demonstrates that SBAR improves numerous aspects of healthcare delivery. A quasi-experimental study showed that the implementation of the SBAR communication tool led to:
- Improved patient safety
- Enhanced quality of care
- Better communication between nurses and physicians
- Reduced communication failures
- More efficient handoff report processes
- Greater confidence among nursing staff when communicating in clinical settings
The Institute for Healthcare Improvement recognizes SBAR as an essential communication strategy that promotes interprofessional communication and ultimately improves patient outcomes.
SBAR Nursing Applications Across Healthcare Settings
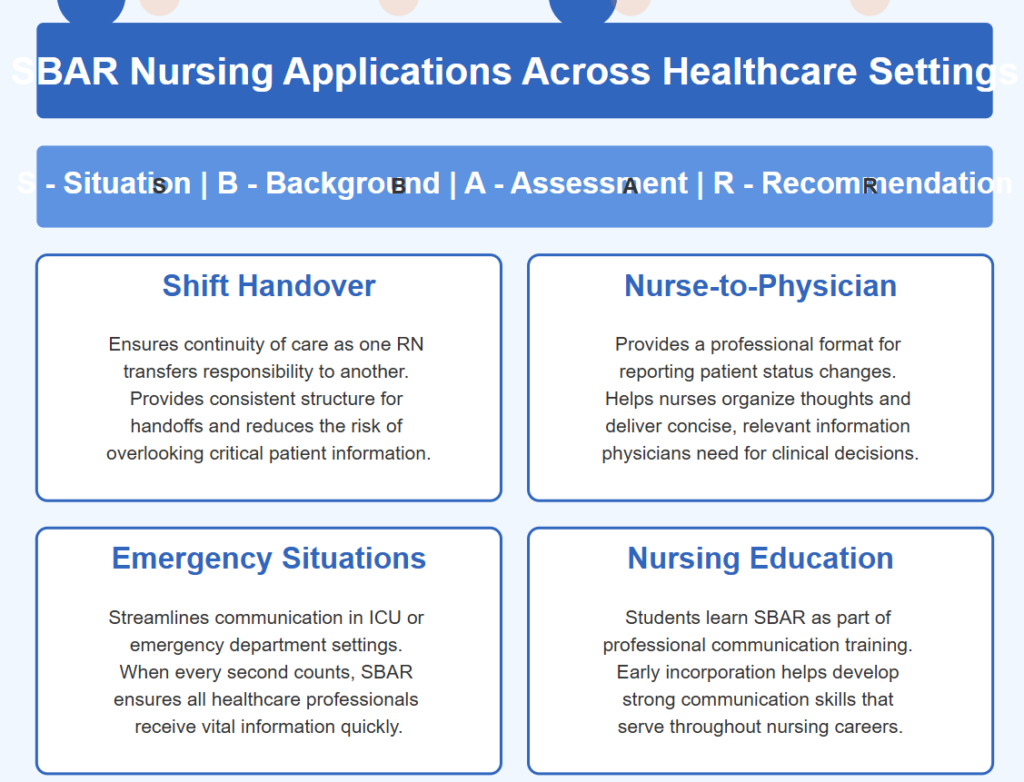
The SBAR framework is versatile and can be adapted for various clinical settings:
Shift Handover
Using the SBAR tool for shift handover ensures continuity of care. When one RN transfers care to another, the handoff communication follows a consistent structure, reducing the risk of overlooking important patient information.
Nurse-to-Physician Communication
When a nurse needs to report to a physician about a change in patient status, SBAR nursing communication provides a professional and efficient format. This structured communication tool helps nurses organize their thoughts and deliver concise, relevant information that physicians need for decision-making.
Emergency Situations
In the intensive care unit or emergency department, SBAR helps streamline communication during critical situations. When every second counts, this standardized communication approach ensures that all healthcare professionals receive the necessary information quickly.
Nursing Education
Nursing students learn the SBAR method as part of their professional communication training. By incorporating this tool early in nursing school, students develop strong communication skills that serve them throughout their nursing profession.
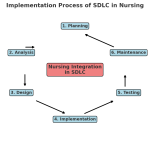
Implementing SBAR in Your Nursing Practice
To effectively incorporate the SBAR communication technique into your daily routine:
- Practice using the SBAR template regularly
- Keep SBAR tool reference cards handy until it becomes second nature
- Encourage fellow nursing staff to adopt this structured communication approach
- Participate in department of nursing initiatives to standardize SBAR use
- Provide feedback on how SBAR helps improve your clinical communication
Frequently Asked Questions
What is an example of a SBAR situation?
A SBAR situation example in nursing typically involves a scenario where a nurse needs to communicate critical patient information concisely to a physician, another nurse, or a healthcare team member. Here is a practical SBAR example in a clinical setting:
Scenario: A post-operative patient is experiencing a sudden drop in blood pressure.
Situation:
“Dr. Carter, this is Nurse Emily from the surgical unit. I am calling about Mr. James, a 65-year-old patient who underwent a total knee replacement yesterday. His blood pressure has suddenly dropped to 88/55 mmHg.”
Background:
“He was stable earlier with a BP of 120/80 mmHg, HR 78, and SpO2 98% on room air. He has a history of hypertension and Type 2 diabetes. He received IV fluids and pain medications during the shift, but no significant changes were noted until now.”
Assessment:
“Currently, he appears pale and slightly diaphoretic. His BP remains low despite elevating his legs, and his heart rate has increased to 105 bpm. Urine output is also reduced in the last two hours.”
Recommendation:
“I recommend assessing him for possible hypovolemia or bleeding. Should I increase his IV fluids, order a stat hemoglobin check, or prepare for further intervention?”
This structured approach ensures clear, efficient, and timely communication between healthcare providers, leading to quicker decision-making and better patient outcomes.
How is SBAR different from traditional nursing reports?
Traditional nursing reports often vary in structure and content depending on the nurse giving the report. SBAR nursing communication, however, provides a consistent framework that ensures all critical information is included every time. This standardized communication tool focuses specifically on relevant information needed for clinical decision-making, eliminating extraneous details that can distract from the key issues.
When should nurses use the SBAR method?
Nurses should use SBAR to communicate in various situations, including:
- Shift handover reports
- Calling physicians about changes in patient status
- Transferring patients between units
- Communicating with other healthcare professionals during emergencies
- Documenting significant changes in patient condition
- Training nursing students in professional communication
The SBAR tool is particularly valuable during high-stress situations when clear communication is essential.
How can nursing students practice using SBAR?
Nursing school programs typically incorporate SBAR training through:
- Role-playing scenarios with peers
- Simulation labs with standardized patients
- Clinical rotations with preceptor feedback
- SBAR template worksheets to complete during clinical experiences
- Video recording practice sessions for self-evaluation
Regular practice using the SBAR tool helps nursing students develop the communication skills necessary for their future nursing practice.
Does SBAR in nursing replace other forms of documentation?
No, SBAR doesn’t replace comprehensive nursing documentation. Instead, it complements existing documentation by providing a structured communication technique for verbal exchanges. Many healthcare settings incorporate SBAR format into their electronic health records for consistency between verbal and written communication.
How has SBAR improved nursing practice?
According to multiple systematic reviews, implementation of the SBAR communication tool has led to:
- 65% reduction in adverse events related to communication failures
- Improved satisfaction among nurses and physicians
- Enhanced confidence among nursing staff when communicating with physicians
- More efficient handoff processes, saving an average of 7 minutes per shift change
- Better identification of deteriorating patients through consistent assessment reporting
These improvements demonstrate why SBAR nursing communication has become standard practice in healthcare settings worldwide.
{kind=link}