Understanding the Nursing Metaparadigm: Key Concepts, Metaparadigm Concepts, and Nursing Theories for Advancing Nursing Science and Patient Care
The nursing metaparadigm serves as the conceptual foundation of the nursing profession, providing a structured framework that defines the central focus of nursing practice and inquiry. At its core, the metaparadigm of nursing encompasses the essential relationships between the four key concepts—person, health, environment, and nursing—which collectively guide both theoretical development and practical application in patient care. These interconnected elements offer nursing students and professionals a lens through which to understand the complex dynamics of human health, the role of the nurse, and the impact of the environment on patient outcomes.
The evolution of nursing metaparadigms has been closely linked to the progression of nursing knowledge development, shaping not only how care is delivered but also how nursing theories are formulated, tested, and applied in clinical settings. By grounding practice in well-defined nursing metaparadigm concepts, nurses are better equipped to implement effective interventions, promote health, and foster well-being across diverse patient populations. Furthermore, understanding the metaparadigm facilitates the integration of transcultural nursing principles, environmental considerations, and health promotion strategies into everyday nursing practice, ensuring care is both comprehensive and patient-centered.
Historically, the nursing metaparadigm has guided the development of nursing as a disciplined profession, influencing curricula in nursing schools, shaping professional standards, and informing research published in leading journals of nursing. Theoretical frameworks such as self-care deficit theory, theory of human, and other foundational models illustrate how metaparadigm concepts translate into practical strategies that enhance the quality of care. For advanced nursing practice, these frameworks provide a systematic approach to decision-making, intervention planning, and evaluation, emphasizing the integration of theory and practice in all aspects of nursing.
This article aims to provide a comprehensive exploration of the nursing metaparadigm, detailing its core concepts, the interplay of its four key components, and its application in nursing theory and clinical practice. By examining the basis of nursing, key theories, and the historical and contemporary development of metaparadigms, nursing students and practitioners alike can gain a clearer understanding of how these foundational principles guide professional nursing practice, improve patient outcomes, and advance the field of nursing science.

What is the Nursing Metaparadigm?
The nursing metaparadigm represents the highest level of conceptual framework in the nursing discipline, defining the fundamental phenomena of interest that distinguish nursing from other health professions. It serves as a conceptual lens through which the focus of nursing is established, guiding both theoretical development and clinical practice. The nursing metaparadigm is traditionally composed of four central elements—person, health, environment, and nursing—which collectively provide a structured understanding of how nurses interact with patients, families, and communities.
For example, in a clinical scenario involving a patient with chronic heart failure, the person component directs attention to the individual’s physical, emotional, and psychosocial needs; the environment considers factors such as home support, accessibility to healthcare, and socioeconomic conditions; health reflects the patient’s current state and desired outcomes; and nursing encompasses the interventions, assessments, and care strategies implemented. Understanding the domain of the nursing metaparadigm ensures that nursing care is holistic, evidence-based, and responsive to each patient’s unique situation.
Historically, the concept of the nursing metaparadigm has been shaped by nursing scientists such as Fawcett in 1984, who articulated its four central components and emphasized their significance in both theory and practice. Today, the nursing metaparadigm continues to inform the foundation of nursing practice, guiding the development of new nursing models, theories, and professional standards.
Why is the Nursing Metaparadigm Important?
The importance of the nursing metaparadigm lies in its ability to unify the aspects of nursing under a coherent framework, allowing practitioners, educators, and researchers to align their work with the profession’s overarching goals. By providing a clear structure for understanding nursing interventions and patient care priorities, it supports the development of effective nursing care across diverse settings, including acute care, community health, and transcultural nursing contexts.
Consider a nurse in advanced nursing practice working with a multicultural population. Knowledge of the nursing metaparadigm concepts allows the nurse to tailor interventions that respect cultural beliefs, health behaviors, and family dynamics while promoting health and well-being. This framework also underpins the creation of care plans that are comprehensive and adaptable, ensuring safe and responsive care.
Furthermore, the metaparadigm provides the basis of nursing as a profession, differentiating nursing from medicine, public health, and other healthcare disciplines. It encourages nursing inquiry, drives theory development, and informs both nursing philosophy and professional nursing education, ensuring that nurses have a structured understanding of their roles, responsibilities, and the impact of their interventions.
How Does the Metaparadigm Shape Nursing Practice?
The nursing metaparadigm shapes practice by offering a guide for nursing that integrates theoretical knowledge with clinical decision-making. It informs the nursing process, including assessment, diagnosis, planning, intervention, and evaluation, ensuring that care is patient-centered and evidence-based. Each component of the metaparadigm serves a practical function:
- Person: Recognizing the individuality and holistic needs of patients.
- Health: Defining goals related to wellness, recovery, or management of chronic conditions.
- Environment: Addressing external and internal factors that affect patient health.
- Nursing: Determining appropriate interventions and professional responsibilities.
For instance, in applying the self-care deficit theory to patients recovering from stroke, nurses assess patients’ ability to perform daily activities (person), set achievable goals for functional independence (health), modify home or hospital settings to ensure a safe environment, and deliver care interventions that restore autonomy (nursing). By grounding practice in the foundation of nursing knowledge development, the metaparadigm enables nurses to provide care that is systematic, holistic, and tailored to individual patient needs.
What Are the Key Components of the Nursing Metaparadigm?
The key components of the nursing metaparadigm—person, health, environment, and nursing—represent the essential elements that define the profession and guide both theory and practice. Each component has unique implications:
- Person: Central to nursing, this component focuses on the individual as a holistic being, including physical, emotional, spiritual, and social dimensions. For example, transcultural nursing theory emphasizes understanding cultural context to provide individualized care.
- Health: Health encompasses the dynamic state of well-being, ranging from illness management to health promotion. Nursing interventions aim to enhance quality of life, support recovery, and foster preventive care.
- Environment: The physical environment, social surroundings, and community resources are all considered when planning care. Environmental factors significantly influence outcomes, as demonstrated in environmental theory, which links surroundings to patient recovery and safety.
- Nursing: This component addresses the practice of nursing, professional roles, and nursing interventions that ensure effective patient care. It also reflects the art and science of nursing, integrating knowledge from various nursing paradigms and theories, such as the theory of human and nursing need theory, into practical application.
Collectively, these components establish a comprehensive framework that informs clinical nursing, research, and professional nursing practice, ensuring that care is both systematic and compassionate. By understanding these elements, nurses can better navigate complex patient scenarios, design effective interventions, and contribute to advancing nursing science.
Core Concepts of the Nursing Metaparadigm
The nursing metaparadigm articulates the broadest conceptual boundaries of the discipline and gives nurses, educators, and researchers a shared vocabulary for describing what nursing is about. At its most widely accepted, the metaparadigm comprises four core concepts — person, health, environment, and nursing — each of which frames a distinct but interdependent domain of concern for the profession. These concepts function together to direct inquiry, guide curriculum design, and shape clinical decision-making; they are the conceptual scaffolding that allow nursing to situate its knowledge, values, and interventions within a coherent professional identity. Fawcett’s influential exposition of the metaparadigm remains a foundational reference in this discussion.
What Are the Four Key Concepts?
The four canonical concepts are:
- Person: the recipient(s) of nursing care — individuals, families, groups, or communities — understood holistically (physical, emotional, social, cultural, and spiritual dimensions).
- Health: a dynamic state that ranges across wellness, illness, adaptation, and recovery; health is both an outcome and an organizing goal of nursing interventions.
- Environment: all external and internal conditions that affect the person’s state of health — physical surroundings, social relationships, cultural norms, economic conditions, and built environment. Recent scholarship has emphasized the environment domain as under-examined yet crucial to outcomes. PMC
- Nursing: the actions, roles, obligations, knowledge base, and professional values that characterize the discipline — from assessment and clinical reasoning to advocacy and health-promotion activities.
Each concept is broad by design so that diverse theories and models can map onto the metaparadigm while preserving nursing’s distinctiveness from other health professions. For example, in a community vaccination program the person is the community served, health is both population immunity and reduced disease burden, environment includes access barriers and misinformation circulating on social media, and nursing encompasses outreach, education, and administration of vaccines.
How Does Person Influence Nursing Practice?
Understanding “person” as holistic and contextual transforms nursing practice from task-oriented care to relationship-centered care. When nurses recognize patients as individuals with unique values, cultural backgrounds, and capacities, assessments shift beyond signs and symptoms to include personal goals, beliefs, resources, and vulnerabilities. Practically, this affects every step of the nursing process — for instance, goal-setting becomes collaborative rather than prescriptive, and education plans are culturally tailored rather than generic.
Example: an older adult with limited English proficiency and diabetes will need an education plan that accounts for language, food culture, health literacy, and family roles. A nurse who attends to these person-level factors will likely design more realistic self-management goals and use interpreters or culturally adapted materials to support adherence.
What Role Does Environment Play in Nursing?
The environment shapes risk, recovery, and the feasibility of nursing interventions. Environmental factors include physical elements (lighting, noise, air quality), social determinants (housing, income, caregiver support), and institutional structures (staffing, policies, equipment). Environmental theory and adaptation-focused models highlight how modifying the environment can be as therapeutically important as direct clinical interventions. For example, modifying a patient’s home to remove fall risks or arranging community supports can prevent rehospitalization and improve functional outcomes. Contemporary literature calls for deeper attention to environmental domains because they frequently explain variation in outcomes that cannot be accounted for by clinical treatment alone.
Why is Health a Central Concept?
Health functions as the primary outcome orientation for nursing — it is what nurses ultimately seek to preserve, restore, or enhance. Importantly, “health” in nursing is multi-dimensional (physical, mental, social) and highly contextual: health goals differ if the priority is curative treatment, chronic disease management, palliative comfort, or community resilience. Nursing’s strength lies in translating broad health goals into individualized, measurable care plans (e.g., blood pressure control, pain reduction, improved function, increased participation in activities valued by the person). By framing interventions around meaningful health outcomes, nursing bridges bedside care and systems-level health promotion.
How Does Nursing as a Discipline Fit In?
“Nursing” in the metaparadigm denotes both the set of actions (assessment, planning, intervention, evaluation) and the profession’s knowledge base and values. As a discipline, nursing synthesizes biological, psychosocial, and behavioral sciences into practiceable knowledge. This synthesis is manifest in nursing models and the nursing process: nurses assess holistically, formulate nursing diagnoses, set collaborative goals, enact targeted interventions, and evaluate progress. The discipline’s identity is reinforced by professional standards, education pathways, and scholarship that link practice to a growing evidence base. Nursing thus occupies a unique role: it mediates between scientific knowledge and individualized human care.
How Do These Concepts Interact with One Another?
The metaparadigm concepts are not isolated boxes — they interact dynamically. Person and environment interact when social supports buffer stress; environment and health interact when poor housing conditions exacerbate respiratory disease; nursing mediates these interactions through interventions that alter the environment, enable self-management, or advocate for resources. The interactional view encourages systems thinking: a seemingly clinical problem (e.g., medication nonadherence) often has environmental or person-level explanations (cost, understanding, cultural beliefs) that must be addressed to achieve health outcomes.
Example: a patient with COPD readmitted after discharge. A metaparadigm-informed assessment might reveal inadequate home heating (environment), low health literacy (person), and limited follow-up (nursing/system). Effective nursing care then targets all three domains — arrange heating assistance, provide teach-back education, and coordinate community nursing visits — to reduce readmission risk.
What Examples Illustrate These Core Concepts in Action?
- Postoperative care pathway: Person = surgical patient with comorbidities; Health = prevention of infection and restoration of function; Environment = operating room sterility and ward staffing levels; Nursing = pain management, wound surveillance, early mobilization. Coordinated nursing interventions prevent complications and speed recovery.
- Community hypertension program: Person = patients in a low-income neighborhood; Health = blood pressure control; Environment = food access, safe spaces for exercise; Nursing = screening clinics, health education, referral to social supports. Addressing environmental barriers enhances clinical outcomes.
- Palliative care consultation: Person = patient and family values; Health = comfort and quality of life; Environment = home or hospice setting; Nursing = symptom assessment, family support, coordination with interdisciplinary team. Nursing integrates person-centered goals with environmental supports to uphold dignity and relief.
Exploring the Metaparadigms of Nursing Theory
Nursing theory and metaparadigms are tightly coupled: metaparadigms (person, health, environment, nursing) provide the broad conceptual scaffold on which nursing theory is built. Theories translate that scaffold into testable, practice-relevant propositions — explaining relationships between concepts, guiding assessment and intervention, and suggesting measurable outcomes. A clear understanding of major nursing theories helps nurses recognize how different theoretical lenses emphasize particular metaparadigm elements and therefore shape practice, education, and research in distinct ways.
What Are the Major Theories in Nursing?
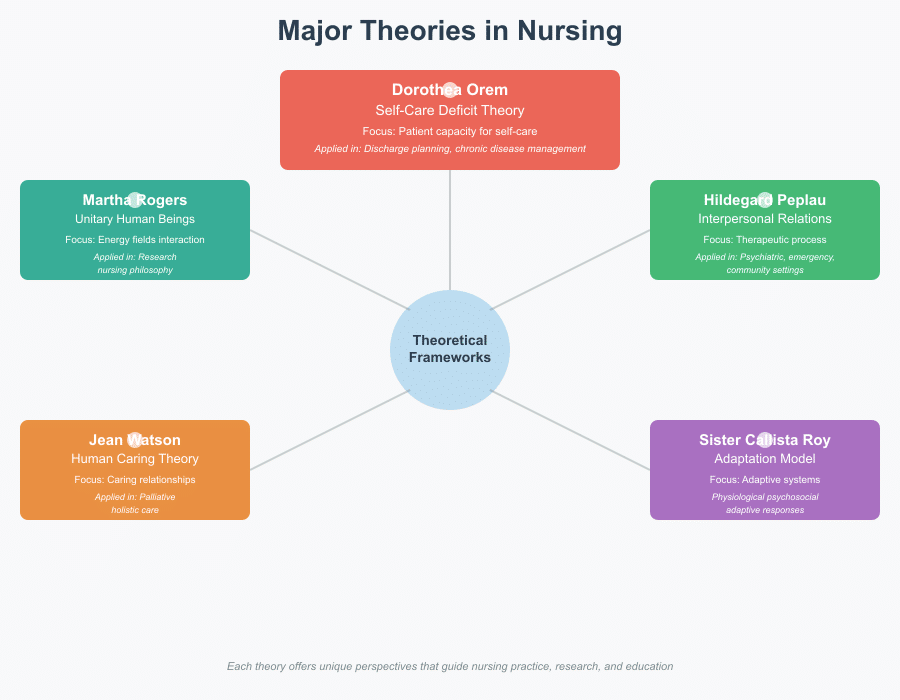
Nursing has generated a rich set of theoretical frameworks that vary in scope and purpose. Some of the most influential include:
- Dorothea Orem’s Self-Care Deficit Theory — centers on patients’ capacity for self-care and the nurse’s role in supporting deficits, frequently used in discharge planning and chronic disease management.
- Hildegard Peplau’s Theory of Interpersonal Relations — frames nursing as a therapeutic interpersonal process; widely applied in psychiatric, emergency, and community settings where nurse–patient relationship is central.
- Sister Callista Roy’s Adaptation Model — views patients as adaptive systems and guides interventions that promote adaptive responses across physiological and psychosocial modes.
- Jean Watson’s Theory of Human Caring (Carative Factors) — emphasizes caring relationships, transpersonal caring, and the moral center of nursing practice; influential in palliative and holistic care.
- Martha Rogers’ Science of Unitary Human Beings (Health as Expanding Consciousness) — conceptualizes human beings and environment as energy fields in constant interaction; used in research and philosophy of nursing.
These and other frameworks (Neuman, Leininger, Benner, etc.) provide a repertoire of lenses nurses can apply depending on clinical goals, setting, and patient needs.
Example: A community nurse using Orem will focus on assessing and building self-management skills for diabetic patients (metaparadigm: person + health + nursing). In contrast, a hospice nurse applying Watson’s caring theory will prioritize presence, meaning-making, and comfort (metaparadigm: person + nursing + environment).
How Do Theories Evolve Over Time?
Nursing theories evolve through cycles of conceptual refinement, empirical testing, critique, and synthesis. Early contributions (e.g., Florence Nightingale’s environmental ideas) established practice-oriented prescriptions; mid-20th century theorists formalized conceptual models; late 20th and 21st century scholarship has focused on empirical validation, contextual adaptation, and integration with interdisciplinary science. Evolution is driven by changes in healthcare delivery, sociocultural shifts, methodological advances, and policy imperatives — for example, the rise of evidence-based practice and population health has encouraged mid-range theory development that is directly testable in clinical studies. Systematic reviews and historiographic work document these shifts and argue for iterative refinement rather than wholesale replacement of useful constructs.
Example: The original tenets of a grand theory (e.g., Roy) have been operationalized in nursing research on adaptation, producing validated intervention components (education, coping strategies) that now appear in clinical guidelines — an instance of theory moving from conceptual to practical application.
What Are the Differences Between Grand and Middle-Range Theories?
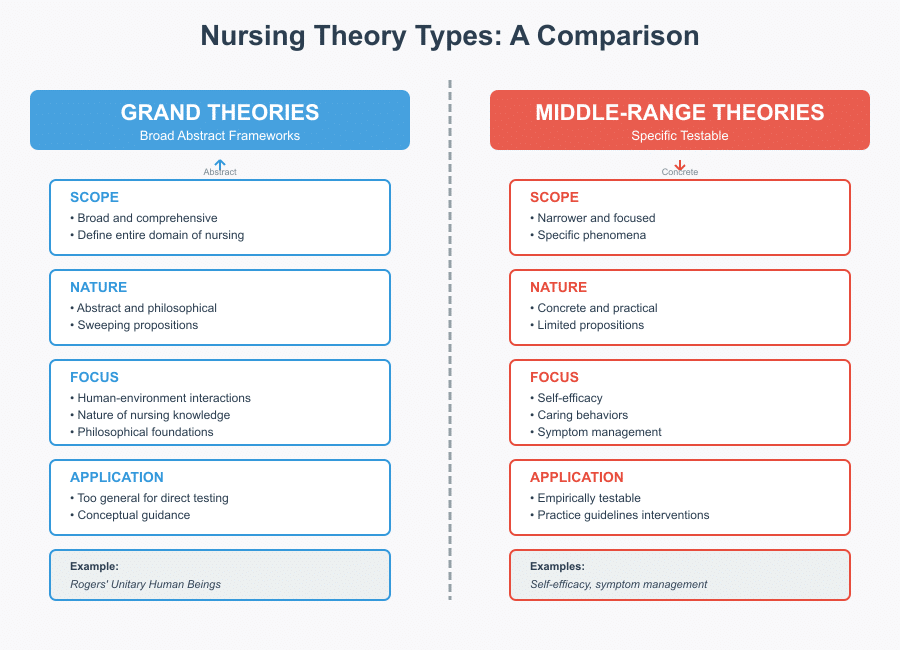
- Grand theories are broad, abstract frameworks that define the domain and philosophical foundations of nursing (e.g., Rogers’ unitary human beings). They articulate sweeping propositions about human-environment interactions and the nature of nursing knowledge, but they are often too general for direct empirical testing.
- Middle-range theories are narrower in scope, focusing on specific phenomena (e.g., self-efficacy, caring behaviors, symptom management). They are explicitly designed to be empirically testable and to inform practice guidelines, measurement development, and intervention studies.
Because middle-range theories bridge grand theory and bedside practice, they are particularly valuable for applied research and curriculum design. Nursing scholars often recommend a multi-level approach: grand theory to orient values and mission, middle-range theory to design interventions and evaluations.
Example: Using a middle-range theory of discharge readiness allows development of a validated assessment tool that frontline nurses can use and researchers can evaluate for predictive validity.
How Do Metaparadigms Influence Nursing Education?
Metaparadigms structure nursing curricula by clarifying what students must know about persons, health, environment, and nursing. In practice, educators map learning outcomes, clinical objectives, and simulation scenarios to metaparadigm elements: assessment skills (person), health promotion and pathophysiology (health), environmental safety and systems thinking (environment), and clinical reasoning and caring practices (nursing). Studies of nursing students’ perceptions show that explicitly teaching metaparadigm frameworks enhances conceptual understanding and helps students connect theory with clinical decision-making. Educators also use metaparadigms to scaffold professional values, ethics, and interprofessional competencies across pre-licensure and advanced programs.
Example: A curriculum sequence might pair a lecture on the Roy Adaptation Model with a community health placement where students assess family adaptation after a natural disaster — aligning theory with experiential learning.
What Role Do Metaparadigms Play in Research?
Metaparadigms guide research questions, variable selection, and interpretation of findings by clarifying which aspects of human experience are central to inquiry. They help researchers justify conceptual models, choose appropriate outcomes, and situate studies within nursing’s intellectual tradition. In mixed-method and intervention research, metaparadigm clarity improves construct validity (e.g., ensuring a “health” outcome is operationalized consistently), informs instrument development, and supports cross-study synthesis. Nursing research’s maturation — from descriptive studies to sophisticated multi-site trials and theory-driven implementation science — reflects this tighter linkage between metaparadigm thinking and methodological rigor.
Example: A study testing a nurse-led home-visit intervention might explicitly anchor its hypotheses in the metaparadigm (environmental modifications → improved functional health), measure environmental variables, and evaluate nursing activities as mediators of outcomes.
Applying the Nursing Metaparadigm in Practice
The nursing metaparadigm (person, health, environment, nursing) is more than an abstract framework — it is a practical tool that organizes assessment, planning, intervention, and evaluation so nursing care is holistic, theory-driven, and outcome-focused. Applying the metaparadigm means deliberately using its four components to shape clinical reasoning, select interventions, coordinate care, and measure results. When nurses explicitly map clinical problems to metaparadigm domains, they not only broaden the range of potential solutions but also improve the clarity and coherence of care plans.
How Can Nurses Utilize the Metaparadigm in Patient Care?
- Structure assessment around the four concepts.
Use assessment templates that capture person-centered data (values, goals, functional status), health status (labs, symptoms, functional goals), environmental influences (home safety, social supports, institutional policies), and nursing roles (education needs, coordination tasks). For example, a comprehensive admission assessment for an older adult should include mobility and ADL ability (person), current disease control and medication effects (health), home stairs or caregiver availability (environment), and anticipated nursing needs for discharge planning (nursing). Anchoring each data point to a metaparadigm element improves completeness and promotes targeted interventions. - Use the metaparadigm to generate nursing diagnoses and care plans.
Framing problems within the metaparadigm clarifies whether an issue is primarily person-related (e.g., impaired coping), health-related (e.g., uncontrolled pain), environment-related (e.g., unsafe home), or nursing-related (e.g., need for teaching). This mapping makes it easier to select evidence-based interventions and set measurable outcomes. For instance, a nursing diagnosis of “self-care deficit” can be linked directly to Orem’s work and translated into progressive self-management goals and specific nursing actions. - Design multimodal interventions that span domains.
Many complex problems require combined approaches — education and skill-building for the person, clinical treatment for health problems, environmental modification, and nursing coordination. In heart failure management, for instance, nurses apply education (person), medication titration and symptom monitoring (health), home adaptations and transportation support (environment), and transitional care coordination (nursing). Research shows interventions that address both clinical and environmental factors have higher effectiveness. - Use theory-informed tools for practice and evaluation.
Adopt validated assessment tools and care pathways based on middle-range theories (discharge readiness, coping scales, fall-risk tools). These instruments transform broad metaparadigm concepts into operational measures and make outcomes auditable. Where possible, align documentation fields in electronic health records with metaparadigm elements to support data-driven quality improvement. - Advocate and modify the environment.
Nurses are uniquely positioned to identify environmental barriers to health — staffing patterns, equipment deficits, patient living conditions — and to advocate for system changes. Evidence links favorable nursing practice environments with better patient outcomes and reduced mortality; hence, metaparadigm-informed advocacy for environmental change is both a professional and evidence-based activity.
What Are Some Real-Life Scenarios Illustrating the Metaparadigm?
Scenario 1 — Reducing Readmissions after COPD Exacerbation
- Person: assess health literacy and smoking status; involve family in education.
- Health: optimize inhaler technique, oxygen use, and medication reconciliation.
- Environment: identify home triggers (smoke exposure) and access to follow-up care.
- Nursing: coordinate home visits, ensure follow-up appointments, and teach self-management.
Outcome: programs that integrate these domains (clinical care + home support) reduce readmissions.
Scenario 2 — Preventing Falls in an Acute Ward
- Person: evaluate balance, vision, medications that increase fall risk.
- Health: treat orthostatic hypotension or manage delirium.
- Environment: ensure adequate lighting, remove trip hazards, provide mobility aids.
- Nursing: conduct regular toileting rounds, implement hourly safety checks, and educate staff and family.
Outcome: multifactorial approaches targeting person + environment + nursing processes yield larger reductions in fall rates than single interventions.
Scenario 3 — Community Hypertension Outreach
- Person: cultural beliefs about medicine and diet; willingness to engage.
- Health: baseline BP control and comorbidities.
- Environment: food deserts, unsafe streets, and clinic access.
- Nursing: community screening, tailored education, referrals to social services.
Outcome: addressing environmental barriers improves adherence and population-level BP control more than clinic-only approaches.
How Can Understanding the Metaparadigm Improve Patient Outcomes?
- Promotes comprehensive solutions. Rather than treating isolated symptoms, metaparadigm-informed practice reveals upstream causes (social determinants, environment) and expands intervention options, which increases the likelihood of durable improvement.
- Improves care coordination. Mapping roles and responsibilities against metaparadigm domains clarifies when to involve interdisciplinary partners (social work, physiotherapy, community nursing), improving continuity and reducing gaps that undermine outcomes.
- Supports measurement and quality improvement. Operationalizing metaparadigm elements in protocols and documentation enables tracking of meaningful outcomes (e.g., functional status, readmission rates, patient-reported health), facilitating targeted quality initiatives. Studies link positive nursing practice environments and comprehensive, theory-informed interventions to better patient safety and lower mortality.
- Enhances patient-centeredness and adherence. Person-focused assessment and shared goal-setting increase engagement and adherence; when patients see care addressing their lived environment and values, outcomes improve.
Challenges and Future Directions in Understanding the Nursing Metaparadigm
Nursing’s metaparadigm remains a powerful organizing framework, yet its translation into everyday education, research, and clinical practice faces real obstacles. Addressing these challenges is essential if nursing is to sustain its conceptual clarity while responding to rapidly changing health systems, population needs, and scientific advances.
What Challenges Do Nurses Face in Applying the Metaparadigm?
- Conceptual ambiguity and fragmentation.
Although the four metaparadigm concepts (person, health, environment, nursing) are widely taught, their definitions vary across theorists and curricula. This variation produces inconsistent application in practice and research — for example, “environment” may be interpreted narrowly as physical surroundings in one curriculum and broadly as sociopolitical determinants in another. The lack of shared operational definitions undermines measurement and cross-study synthesis. - Theory–practice gap.
Many nurses report that theories feel abstract and removed from clinical realities such as staffing shortages, time constraints, and complex comorbidities. This gap reduces uptake of theory-based interventions on the bedside, with nursing staff defaulting to task-oriented care rather than theoretically grounded, holistic interventions. - Educational constraints.
Overloaded curricula and competing accreditation requirements can limit depth of theory instruction in school of nursing programs. Students may graduate with strong technical skills but limited experience applying metaparadigm thinking to complex clinical situations. - Resource and system barriers.
Environmental limitations (unit layout, equipment access, staffing ratios) and organizational culture can impede metaparadigm-informed interventions — for example, nurses may identify environmental hazards that require interdisciplinary or policy-level solutions beyond their immediate control. - Measurement and evidence challenges.
Translating broad metaparadigm constructs into reliable, valid measures is difficult. Outcomes like “person-centeredness” or “environmental fit” require multi-dimensional instruments and mixed-method approaches that demand time and methodological expertise. - Cultural and contextual variability.
Global and local cultural differences mean that metaparadigm components must be adapted carefully; a one-size-fits-all model risks marginalizing certain populations if cultural values and health constructs are not honored.
How Can Nurses Address These Challenges?
- Clarify and operationalize constructs locally.
Nursing teams and educators can co-create pragmatic definitions of metaparadigm elements for their settings — for instance, defining “environment” to include specific social determinants tracked by the unit (housing instability, caregiver availability). Local operational definitions enable consistent documentation and evaluation. - Embed theory into clinical tools and workflows.
Convert metaparadigm concepts into checklists, assessment fields in electronic health records, and care-pathways. For example, add an “environmental risk” field to discharge forms so social and physical barriers are systematically identified and referred. - Bridge theory and practice in education.
Use simulation, case-based learning, and clinical practicums explicitly mapped to the metaparadigm so students practice linking theory to decision-making. Faculty mentorship programs and bedside teaching that model metaparadigm reasoning help graduates carry concepts into practice. - Promote interdisciplinary collaboration and advocacy.
Because many metaparadigm challenges are structural, nurses must partner with social workers, public health professionals, administrators, and policy-makers to address upstream determinants. Nursing leadership can translate clinical insights into organizational change (e.g., safety renovations, community partnerships). - Invest in measurement and translational research.
Researchers should prioritize development and validation of instruments that operationalize metaparadigm constructs and test theory-driven interventions using rigorous designs (mixed methods, implementation science). This strengthens the evidence base and facilitates uptake. - Cultivate reflective and practice-based scholarship.
Encourage staff nurses to engage in small-scale practice improvement projects grounded in metaparadigm thinking; dissemination of successful initiatives builds a practical knowledge base and demonstrates feasibility.
Example: A hospital unit struggling with high readmission for heart failure can adopt a metaparadigm-informed bundle: structured assessment (person), standardized clinical targets (health), a home-safety/environment checklist with social work referrals (environment), and a nurse-led transitional care protocol (nursing). Evaluation can track readmission, patient-reported self-efficacy, and uptake of referrals — demonstrating how theory maps to measurable outcomes.
What Is the Future of Nursing Theories and the Metaparadigm?
- Convergence with implementation science and evidence-based practice.
Nursing theory will increasingly pair with implementation frameworks to test how metaparadigm-informed interventions scale in real-world settings. Middle-range theories that are explicitly testable will remain central to demonstrating practical impact. - Integration with digital health and big data.
Electronic health records, wearable sensors, and population health datasets create opportunities to operationalize metaparadigm constructs at scale (e.g., mapping environmental risk using geospatial data). Data-driven insights can refine theoretical models and reveal patterns not visible at the bedside. - Emphasis on context-sensitive, culturally responsive models.
The future will favor adaptive models that honor cultural variation and co-production with communities. Culturally grounded modifications of existing theories (for instance, integrating indigenous health perspectives) will strengthen global applicability. - Interdisciplinary and systems-level theorizing.
Nursing theory will interface more with social sciences, public health, and environmental science to account for complex systems influencing health. This broadening will help the metaparadigm address large-scale challenges such as climate change, health inequities, and pandemics. - Education innovation and lifelong learning.
Curricula in school of nursing programs will increasingly use integrated, longitudinal approaches that revisit metaparadigm concepts across clinical rotations, advanced practice tracks, and continuing professional education to support sustained theory–practice integration. - A renewed focus on middle-range theories and practice-based models.
As healthcare demands actionable solutions, middle-range and practice-based theories that clearly link to interventions and outcomes will be prioritized for research funding, guideline development, and quality improvement.
Example (future-facing): A collaborative program between a school of nursing and a public health department uses neighborhood-level environmental indices (air quality, green space, access to healthy food) combined with patient-reported data to design nurse-led outreach. The program tests a theoretically grounded model predicting respiratory exacerbations and demonstrates reduced emergency visits through targeted environmental and nursing interventions — illustrating how metaparadigm-informed research, data, and practice converge.
Conclusion
The nursing metaparadigm remains one of the most enduring and unifying frameworks in the discipline of nursing. By centering practice on the four foundational concepts—person, environment, health, and nursing—it provides a clear lens through which nurses can understand human experiences, deliver holistic care, and uphold the philosophical roots that define the profession. Whether applied in acute care, community health, transcultural settings, or advanced nursing practice, these metaparadigm concepts guide nurses in making informed decisions that honor patient individuality while promoting safety, healing, and dignity.
The evolution of nursing theories, from Nightingale’s environmental theory to contemporary frameworks like transcultural nursing and the self-care deficit theory, demonstrates how the metaparadigm continues to expand and adapt to societal changes, technological innovation, and the growing complexity of the health-care landscape. As nursing students, practicing clinicians, and future nursing theorists engage with these ideas, they also contribute to the continuous refinement of nursing paradigms and the overall history of nursing.
In today’s dynamic care environments, understanding the metaparadigm is not optional—it is essential. It strengthens critical thinking, enhances patient advocacy, improves interdisciplinary communication, and elevates the standard of care provided across all settings. Most importantly, it empowers every nurse to see beyond tasks and interventions, recognizing the profound human experience at the center of every clinical encounter.
As the profession continues to grow, the nursing metaparadigm will remain a guiding compass—shaping education, research, and practice while inspiring new theories that reflect the diverse and evolving needs of global populations.
Frequently Asked Questions
What are the 4 nursing theories of Metaparadigm?
The four components commonly referred to as the nursing metaparadigm (often mistaken as “theories”) are:
- Person – the individual, family, or community receiving care.
- Environment – the internal and external conditions affecting the person.
- Health – the person’s level of wellness or well-being.
- Nursing – the actions, interventions, and role of the nurse.
What are the 4 key concepts of nursing?
The four key concepts are the same as the metaparadigm elements:
- Person
- Environment
- Health
- Nursing
These concepts provide a universal foundation for all nursing theories.
What are the 5 essential components of her theory?
If referring to Florence Nightingale’s Environmental Theory, the five essential components traditionally emphasized are:
- Pure air
- Pure water
- Efficient drainage
- Cleanliness
- Light (especially sunlight)
These environmental elements promote healing and prevent illness.
Which of the four concepts common in all nursing theories is the most important to nursing?
While all four concepts are interconnected, “Person” is widely considered the most important because:
- Nursing is fundamentally person-centered.
- All care decisions revolve around the needs, values, and experiences of the individual.
- Without understanding the person, the nurse cannot apply the other concepts effectively.