N 3661 Exam 1 Exam Blueprint – Med Surg Exam 1 blueprint nurs 3661
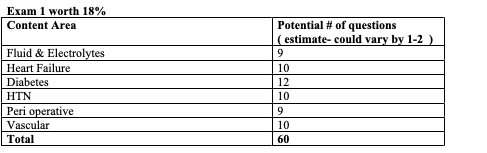
The focus of the N3561 exams is nursing management (Med Surg Exam 1 blueprint nurs 3661. This will mean you need to recognize risk factors (what can they nurse teach about here), expected findings, signs of complications, how is this condition/disease managed (medications , diet , exercise , etc…). So, when you look at the content areas – think assessment, planning, intervention and evaluation.
Perioperative Nursing
- Explain the nurse’s responsibilities preoperatively and during surgery.
Pre-op responsibilities
- Assessment (includes vitals)
- Ensure that ordered diagnostic procedures are done and provider is notified of abnormal results (labs, X-rays, EKG’s).Witness informed consent.Patient in gownAllergy/ID bands placed on pt.Perform any required bowel prep. Perform any required skin prep. Start IV (at least an 18 gauge) Give ordered pre-op meds.Ensure patient has been NPO.Remove all jewelry, dentures, prosthetics, make-up, nail polish, glasses, contacts.Pt teaching about what to expect after surgery.Ask about blood thinners (aspirin, Plavix, lovenox, etc.)Patient uses restroom prior to ORDocumentationIntra-op responsibilitiesRoom prep (privacy, infection prevention, safety)Transfer pt to OR suite (verify pt identity, transfer pt safely)Surgical time-out (before anesthesia given) Pt confirms name & DOB.Operative procedure and procedure sitePatient consent (verbal)Compare hospital ID # with pt armband and chart.Maintain sterile field.Sponge/instrument count. Position pt for optimal alignment Prevent chemical injury.Electrical equipment safety.Give meds safely.Monitor vitals.
- Monitor blood loss and urine output.
- Identify the purpose and components of preoperative nursing assessment and interpret the significance of data related to the patient’s health status and risk.
- Vital signs (establishes baseline and is safety precaution)
- Home medications (prescription, OTC, herbal supplements) Especially blood thinners (including aspirin) and beta blockers – reduced nonfatal MIs in highrisk patients undergoing elective surgery. Therefore, pts. Who are already on beta blockers should continue to take them during the perioperative period.
- Allergies to drugs, foods, or latex (allergy to kiwi, avocado, bananas, [[or balloons may indicate latex allergy)
- Previous surgical history/reactions to anesthesia
- Labs/X-ray/EKG
- Urinalysis- kidney fx, rule out infection.
- Blood type and crossmatch- if pt needs transfusion.
- CBC- hydration, anemia, infection/immune status
- Pregnancy test- fetal risk
- Clotting studies- PT, INR, aPTT, platelet count
- Electrolyte levels (usually a BMP or CMP)- electrolyte imbalances
- Serum creatinine and BUN- kidney fx
- ABG’s (per ATI book) oxygenation status
- Chest x-ray- heart and lung status
- EKG- baseline, check for dysrhythmias, hx of cardiac disease, done on all pt’s over 40 (per ATI)
- Nutritional status –
- obesity, weight loss, malnutrition, deficiencies in specific nutrients,
- metabolic abnormalities (nutrition affects healing. Table 17-2 on pg 425 talks about specific nutrients)
- Hydration status -dehydration, hypovolemia and electrolyte imbalances can cause significant problems in surgery.
- Dental- do they have dentures or anything removable in their mouth? Any anatomical issues that might make it hard for intubation. Decaying teeth may crumble and go into airway during intubation
- Drug/alcohol use – weakens immune system, can interfere with medications, increases post-op complications, alcoholics tend to be malnourished.
- Respiratory status – infections, resp diseases (asthma, COPD), smoking causes poor wound healing, more surgical site infections, complications the include blood clots and pneumonia.
- Cardiovascular status- ensure pt can tolerate the O2, fluid and nutritional requirements of surgery. Uncontrolled HTN may cause delays in surgery.
- Liver fx– liver metabolizes the medications, if liver sucks, meds can build up and be toxic.
- Kidney fx– kidneys excrete meds, most surgeries are contraindicated on patients with renal problems unless the surgery is absolutely necessary.
- Endocrine fxo
- Diabetes- hypoglycemia can develop from inadequate carbs or too much insulin,
- hyperglycemia can develop from stress of surgery and can increase risk of wound infection.
- Patients who have been on corticosteroids any time in the last year may be at
- risk of adrenal insufficiency. Must be reported to CNRA or anesthesiologist.
- Pt’s with uncontrolled thyroid disorders are at risk of thyrotoxicosis (with hyperthyroid disorders) or respiratory failure (with hypothyroid disorders)
- Immune fx– determines infection and allergies. Immunosuppression can occur with corticosteroid therapy, organ transplant, radiation, chemo, immune system disorders like AIDs and leukemia.
- Psychosocial factors–
- Preoperative anxiety (determine what it’s related to and provide supportive guidance)
- Pt’s support system (how much help do they have or need at home?)
- Pt’s baseline level of functioning and typical daily activities (assist in pt’s care and recovery)
- Pt’s readiness to learn and how they learn (to provide the most affective education)
- Spiritual & cultural beliefs
- We must help the pt obtain the spiritual support they request (within reason of course, no live chickens or goats or anything)
- Ask pt if their spiritual advisor is aware of impending surgery (be careful how you say it because it may make pt’s think that you think they are going to die or something)
- Ask pt which ethnic group they belong to and any customs/beliefs the pt holds about illness and health care providers.
- Joint problems – can impact patient positioning in surgery, don’t want to bend something in a way that it doesn’t bend anymore.
- Special considerations
- Elderly– can have more comorbidities. They have less physiological reserve (ability of an organ to return to normal after a disturbance in its equilibrium). Respiratory and cardiac complications are leading causes of post-op morbidity and mortality in older adults.
- Bariatrico BMI > 30. Obesity increases the risk and severity of complications from surgery.
- Increase in wound infections and dehiscence. Possible restrictions on theability to move.
- Increased cardiac demand.
- Shallow respirations when supine increased risk of hypoventilation and postop pulmonary problems.
- Can have short, thick necks, big tongues, recessed chins, etc that can make them harder to intubate, increase O2 demand and decrease pulmonary reserves.
- Assess for sleep apnea, very common in overweight folks.
- Pt’s with disabilities– assess for need for assistive devices, modifications in
- preop education, additional assistance with positioning and transferring.
- Explain the etiology and nursing assessment with management of post-operative care.
- Objectives are to provide care until pt has recovered from effects of anesthesia (resumes motor and sensory fx), making sure that the pt is oriented, has stable vital signs, and shows no evidence of hemorrhage or other complications.
- Assess – airway, respiratory fx, cardiac fx, skin color, level of consciousness, ability to respond to commands, vital signs (minimum Q15, more frequent if needed), surgical sites, drainage tubes and monitoring lines, IV fluids and meds.
- Airway
- Primary objective- right after surgery, is maintaining ventilation and preventing hypoxemia and hypercapnia.
- Give O2 as prescribed, assess resp rate & depth, ease of respiration, O2 sats, breath sounds.
- Monitor for hypopharyngeal obstruction from lower jaw and tongue blocking airway.o S/S: choking, noisy & irregular respirations, decreased O2 sats, cyanosis (blue, dusky skin color).
o Can try head tilt and chin lift to improve.
- Use hand to feel pt’s breath, just b/c pt’s chest is moving doesn’t mean they are breathing HOB elevated 15 to 30 degrees unless contraindicated.
- If vomiting, turn on the side.
- Suction if needed.
- Cardiac
- Primary post op CV complications are hypotension and shock, hemorrhage, HTN and dysrhythmias.
- Hypotension– blood loss, hypoventilation, position changes, pooling of blood in extremities, side effects of meds.
- Shock-
- Can be classified as hypovolemic, cardiogenic, neurogenic, anaphylactic, and septic.
- Most common is hypovolemic.
- If vomiting, turn on the side.
S/S: pallor; cool, moist skin; rapid breathing; cyanosis of lips, gums, and tongue; rapid, weak, thready pulse; narrowing pulse pressure; low blood pressure; concentrated urine.
- Relieve pain and anxiety –
- usually opioids b/c they provide immediate relief and are short acting so not as much of a risk of prolonged respiratory depression.
- Control nausea/vomiting – treat nausea ASAP to decrease chance of vomiting and aspiration.
- Determine if pt ready to leave PACU (is a critical care unit where the pt’s vital signs are closely observed, pain mgt begins and fluids are given) o Aldrete score (tool to maintain assessment of the post anesthesia pt as they move through their stay in the dept. and in the hospital).assign number of 0, 1,, or 2 to 5. Variables.
- Used to determine if pt is ready to leave PACU (Post Anesthesia Care Unit) o Q15 minutes, pt given score for activity (movement), respiration, circulation (blood pressure), consciousness, and O2 sats. Scores are added and usually if pt scores are below 7, they must stay in PACU. Usually, a score of 7-10 means pt can leave PACU. o ATI list of what nurses should monitor and assess.
- Airway, circulation. Vital signs, positioning, response to anesthesia (sedation, nausea, vomiting), I/O’s, surgical wound/incision site/drainage, pain, mentation (mental activity).
- Choose strategies to prevent postoperative complications. Airway obstruction
- Monitor for S/S of hypopharyngeal obstruction discussed above and intervene.
- Head-tilt/chin-lift.
- Keep resuscitation bag, suction equipment and airway supplies at bedside.
- Notify anesthesiologist,
- Elevate HOB if not contraindicated.
- Give humidified O2,
- Prepare for reintubation with ET tube.
- Hypoxia
- Monitor O2 status and give O2 as prescribed.
- Encourage coughing and deep breathing to prevent atelectasis.
- Elevate HOB and turn Q2 hours to facilitate chest expansion.
- Hypovolemic shock
- Monitor for decreased BP and urinary output, increased heart and respiratory rates, narrowing of pulse pressure and slow cap refill.
- Give O2.
- Supine position with legs elevated.
- IV fluids and vasopressors as prescribed.
- Paralytic ileus
- Monitor bowel sounds. Encourage ambulation.
- Advance diet as tolerated when bowel sounds or flatus are present.
- NG tube placement if needed to empty stomach.
- Give prokinetic agents, such as metoclopramide, as prescribed.
- Wound dehiscence or evisceration.
- Monitor risk factors (obesity, coughing, moving without splinting, poornutritional status, diabetes, infection, hematoma, steroid use).
- If it occurs, call for help, stay with pt, cover wound with sterile towel ordressing that is moistened with sterile saline, do not attempt to reinsert organs, place in low-Fowlers with hips and knees bent, monitor for shock, notify provider STAT.
- DVT-
- Prophylactic treatments:
- low molecular weight heparin.
- low-dose heparin, low dose warfarin.
- anti-embolism stockings.
- pneumatic compression devices.
- range of motion (ROM) exercises.
- early ambulation
- low molecular weight heparin.
- Avoid any pressure behind the knee with a pillow or blanket, can constrict bloodvessels and decrease venous return.
- Don’t let pt’s legs dangle very long.
- Hydration with IV fluids and PO intake
- Other complications listed on last page of powerpoint
- Pulmonary embolism
- Urinary retention
- Infection
- Gastric dilation
- Pneumonia
- Atelectasis
- Describe general discharge teaching for the postop patient.
Teach the patient-
- The purpose, administration, guidelines, and adverse effects of meds
- Activity restrictions (driving, stairs, limits on weightlifting, sexual activity) Dietary guidelines
- Treatment instructions (wound care, catheter, care, use of assistive devices) Emergency contact info and what complications they should report.
Content
Perioperative Care
A. Preoperative Nursing
- Consent
- Medications to avoid
- Teaching
- Medications to avoid
B. Postoperative Nursing
- Prevent complications ( IS, CD&B, ambulation , SCD’s etc..)
- Assessment
C. Discharge Teaching
- potential limitations
- teaching that should occur ( what does the nurse need to cover)
Fluid & Electrolytes
Identify patients at risk for F&E imbalance. Infant age 1 and under and older adults.
Describe the etiology, laboratory, diagnostic findings and nursing as well as collaborative management of persons with fluid and electrolyte imbalances.
II. Fluid & Electrolyte Imbalances
A. Electrolyte imbalances
a. Sodium
- Normal range 135-145
- Hyponatremia – < 135 Signs/symptoms:
- Anorexia, nausea and vomiting, headache, lethargy, dizziness, muscle cramps and weakness, muscle
twitching, seizures, increased pulse, decreased BP,
- Labs:
- Decreased serum and urine sodium, decreased urine specific gravity and osmolality.
- Management.
- Sodium replacement and water restriction management:
- Monitor and Ident. pts at risk.
- Nursing management
- Monitor I&O and daily weight.
- Hypernatremia
- 1. >145
- Signs and symptoms
- Thirst, elevated body temp, swollen dry tongue and sticky mucus membranes, hallucinations, lethargy,
- restlessness, irritability, simple partial or tonic clonic. seizures, pulmonary edema, hyperreflexia, twitching, nausea, vomiting, anorexia, increase pulse and BP.
- Labs
- Increased serum sodium, decreased urine sodium,
- increased urine specific gravity and osmolality
- Nursing management
- Gradual lowering of serum sodium with IV hypotonic solution or isotonic non saline solution
- I&O monitoring.
- Calcium
- Normal range 8.5-10.5 Hypocalcemia – <8.5
- Signs and symptoms
- Numbness, tingling of fingers, toes, and circumoral region.
- Positive Trousseau sign and Chvostek sign.
- seizures, carpopedal spasms, hyperactive deep tendon reflexes, irritability, bronchospasm, anxiety, impaired clotting time,
- ↓ prothrombin, diarrhea,
- ↓BP. ECG: prolonged QT interval and lengthened ST
- Management
- Acute symptomatic
- IV infusion of calcium salts.
- Nutritional therapy
- Vitamin D
- Nurse management
- Monitor pt if severe seizure precautions areimplemented.
- Airway monitored for laryngeal stridor.
- Diet education
- Positive Trousseau sign and Chvostek sign.
- Numbness, tingling of fingers, toes, and circumoral region.
- Hypercalcemia >10.5
- Signs and symptoms
Muscular weakness, constipation, anorexia, nausea and vomiting, polyuria and polydipsia, dehydration, hypoactive deep tendon reflexes, lethargy, deep bone pain, pathologic fractures, flank pain, calcium stones, hypertension. ECG: shortened ST segment and QT interval, bradycardia, heart blocks
- Management
- Aim to decrease calcium level.
- Treating the underlying cause is essential.
- Nurse management
- Increase mobility and encourage fluid intake.
- Unless contraindicated fluids with sodium should be encouraged.
- Encourage adequate fiber intake.
- Monitor cardiac rhythms.
- Nurse management
- Treating the underlying cause is essential.
- Aim to decrease calcium level.
- potassium
- Normal 3.5-5
- Hypokalemia <3.5
- Signs and symptoms
- Fatigue, anorexia, nausea and vomiting, muscle weakness, polyuria, decreased bowel motility, ventricular asystole or fibrillation, paresthesia’s, leg cramps,
- ↓ BP, ileus, abdominal distention, hypoactive reflexes.
- ECG: flattened T waves, prominent U waves, ST depression, prolonged PR interval
- Management
- Oral or IV potassium replacement Nurse Management
- Monitor ECG and for dig toxicity.
- Hyperkalemia – >5
- Signs and symptoms
- Muscle weakness, tachycardia → bradycardia, dysrhythmias, flaccid paralysis, paresthesia, intestinal colic, cramps, abdominal distention, irritability, anxiety.
- ECG: tall, tented T waves, prolonged PR interval and QRS duration, absent P waves, ST depression
- Management
- ECG immediately obtained.
- Kayexalate (poo the potassium away)
- Emergency management
- Hypokalemia <3.5
- Normal 3.5-5
- IV calcium gluconate
- IV regular insulin and a hypertonic dextrose solution
- Nurse management
- Monitor pt and I&O
- Nurse management
- Magnesium
- Normal 1.3-2.3
- Hypomagnesemia – <1.3
- Signs and symptoms
- Neuromuscular irritability, positive Trousseau sign and Chvostek sign, insomnia, mood changes, anorexia, vomiting, increased tendon reflexes, and ↑BP.
- ECG: PVCs, flat or inverted T waves, depressed ST segment, prolonged PR interval, and widened QRS.
- Management
- Mild-diet therapy
- Magnesium salts can be given orally or IV.
- Nurse management. Monitor pt.
- Education
- Hypermagnesemia >2.3
- Signs and symptoms
- Flushing, hypotension, muscle weakness, drowsiness, hypoactivereflexes, depressed respirations, cardiac arrest and coma, diaphoresis.
- ECG: tachycardia →bradycardia, prolonged PR interval and QRS, peaked T waves
- Management
- Avoid magnesium salts on pts with kidney injury.
- In emergent situations IV calcium gluconate is indicated.
- Neuromuscular irritability, positive Trousseau sign and Chvostek sign, insomnia, mood changes, anorexia, vomiting, increased tendon reflexes, and ↑BP.
- Normal 1.3-2.3
B.NO ABG’S (arterial blood gases)
- Fluid Volume Deficit; causes, symptoms and management. Remember BP changes
- know orthostatic BP – how do you do it ? What’s normal ?
- Fluid Volume Excess; causes, symptoms and management.
- Some specific electrolyte disturbances- examples (not an all-inclusive list electrolytelosses secondary GI issue (like an NGT) NO ABG’S (arterial blood gases)
Heart Failure:
Heart Failure
- Causes ( risk factors)
- Clinical Manifestations
- Left-sided HF
- Signs/symptoms
- Dyspnea, orthopnea, nocturnal dyspnea Fatigue
- Displaces apical pulse.
- S3 heart sound (gallop)
- Pulmonary congestion
- Frothy sputum
- AMS
- Manifestations of organ failure such as oliguria
- nocturia
- Nursing management
- Dyspnea, orthopnea, nocturnal dyspnea Fatigue
- Signs/symptoms
- Right-sided HF
- Signs/symptoms
- JVD
- Ascending dependent edema
- Fatigue, weakness
- Nausea and anorexia
- Polyuria at rest (nocturnal)
- Liver enlargement and tenderness
- N 3561 Exam 1 Exam Blueprint
- Weight gain
- Nursing management Medical Management
- labs to monitor.
- BNP
- lytes
- Pharmacologic Therapy
- Diuretics. (Labs to monitor, how do you know the medication was effective)
- Digoxin. (Sign of toxicity, what does the nurse need to monitor)
- HF Plan of Care
- weight management /monitoring signs of exacerbation
- LOOK FOR ABOVE.
- Signs/symptoms
- Left-sided HF
Hypertension:
Identify risk factors associated with primary hypertension.
- Nonmodifiable risks
- Age: over 60 or postmenopausal
- Race: especially African Americans
- Family history
- Gender
- Prehypertension or gestational diabetes
- Modifiable risks
- Overweight or obese
- High sodium intake
- Alcohol use
- Lack of physical activity
- Smoking
- Stress
- Hyperlipidemia
- Race: especially African Americans
- Age: over 60 or postmenopausal
Explain the medical and nursing management of the person with hypertension.
- Lifestyle modifications
- Weight loss (shoot for BMI of 18.5-24.9)
- DASH diet (Dietary Approaches to Stop Hypertension)
- Rich in fruits & vegetables
- Low-fat dairy
- Reduce saturated and total fat.
- Reduce sodium intake to at least < 2400 mg a day, but preferably <1500 mg a day.
- Aerobic activity at least 30 minutes a day, most days of the week
- Reduce alcohol- limit consumption to 2 drinks or less (24 oz beer, 10 oz of wine,
- or 3 oz 80-proof whiskey) per day in most men and 1 drink of less per day in
- women or lighter weight people.
- Medication therapy (they will start on lowest dose, then increase gradually if needed.
- Multiple medications may be needed to reach the target).
- The medications used for treating hypertension decrease peripheral resistance, blood volume, or the strength and rate of myocardial contraction. Initial medication for African American patients and patients over 60 with stage I hypertension is a calcium channel blocker or a thiazide diuretic. Patients with stage I who are not African American and less than 60 are started with an ACE inhibitor or ARB. Patients are initially given low doses of medication. If the blood pressure does not fall less than 140/90 mm Hg, the dose is increased gradually, and additional hypertension medications may be included. When the bp is less than 140/90 for a least 1-year, gradual reduction of the types and doses is considered.
- Diuretics
- Thiazide diuretics (hydrochlorothiazide)
- Usually, the first drug they put people on if they don’t have any other. major issues
- Rich in fruits & vegetables
- DASH diet (Dietary Approaches to Stop Hypertension)
- Weight loss (shoot for BMI of 18.5-24.9)
- Prevents reabsorption of sodium and water Excretes more potassium.
- Monitor for hypokalemia.
- Pt may need to eat more potassium.
- Loop diuretics (furosemide AKA Lasix) Same info as thiazides.
- Potassium-sparing diuretics (spironolactone) Prevent reabsorption of sodium Hold onto potassium.
- Monitor for hyperkalemia.
- ACE Inhibitors (lisinopril and enalapril)
- Prevent angiotensin I from converting to angiotensin II whichprevents vasoconstriction.
- Monitor for hypotension, heart or kidney complications, edema.
- Teach pt to report cough and any signs of heart failure (edema)
- Can cause angioedema, HUGE swollen lips
- Beta blockers (metoprolol and atenolol)
- Decrease cardiac output and block release of renin, leads todecreased.
- Loop diuretics (furosemide AKA Lasix) Same info as thiazides.
vasoconstriction
- Good for unstable angina or MI
- Check bp and PULSE before giving.
Identify the impact of uncontrolled hypertension on other body systems. (renal, cardiac, eyes, etc.…)
- Uncontrolled hypertension can result in a hypertensive crisis. Manifestations include-
- severe headache, extremely high blood pressure greater than 240/120, blurred vision, dizziness, disorientation, and epistaxis.
- Prolonged blood pressure elevation gradually damages blood vessels throughout the body, target organs such as the heart, kidneys, brain, and eyes.
- The typical outcome of Uncontrolled hypertension is MI, heart failure, chronic kidney disease, stroke, and impaired vision.
- Hypertrophy of the left ventricle of the heart may occur as it works to pump blood against the elevated pressure.
- severe headache, extremely high blood pressure greater than 240/120, blurred vision, dizziness, disorientation, and epistaxis.
Identify which evaluation(s) would indicate a therapeutic response to the medical and nursing interventions.
- Reports knowledge of disease management sufficient to maintain adequate tissue perfusion such as
- The patient maintains a blood pressure less than 140/90 mm Hg with lifestyle modifications and medications.
- Demonstrations no symptoms of angina, palpitation, or vision changes. Has stable BUN and serum creatinine levels.
- Has palpable peripheral pulses.
- Adheres to the self-care program such as abstains from tobacco and alcohol intake, adheres to dietary regimen, exercise regularly, takes medication.
- Keeps follow up appointments, and measure bp routinely.
- Has no complications such as no changes in vision.
- exhibits no retinal damage on vision testing.
- reports no dyspnea or edema.
- maintain pulse rate and rhythms and respiratory rate with normal ranges.
- maintain urine output consistent with intake.
- has renal function test results within normal range.
- demonstrates no motor, speech, or sensory deficits.
- and reports no headaches, dizziness, weakness, change in gait, or falls.
- The patient maintains a blood pressure less than 140/90 mm Hg with lifestyle modifications and medications.
Identify and discuss what is/are the priority teaching(s) to patients with hypertension.
- Express the importance of adhering to the medication regimen.
- Encourage the patient to keep all appointments with the provider to monitor efficacy of pharmacological treatment and possible electrolyte imbalance.
- Encourage potassium-rich foods if the patient is taking a potassium-depleting diuretic.
- Instruct patients who are taking antihypertensives to change positions slowly, and to be careful when getting out of bed, driving, and climbing stairs.
- Patients should rise slowly to prevent postural hypotension.
- Patients should not stop their medications abruptly. Smoking cessation and stress reduction.
- Patients should be taught how to monitor BP at home.
- Encourage the patient to keep all appointments with the provider to monitor efficacy of pharmacological treatment and possible electrolyte imbalance.
Effect on organs macrovascular vs microvascular (this is complications)
- Potential complications include left ventricular hypertrophy, MI, heart failure, TIAs, cerebrovascular disease (stroke or brain attack), renal insufficiency and chronic kidney disease, and retinal hemorrhage.
Patient teaching- Diet- what kind? What does the nurse need to teach about?
Dash Diet:
- consume a diet rich in fruits, vegetables, low-fat dairy products with a reduced content of saturated fat.
- monitor for hyperkalemia with salt substitute use.
- Consume less than 2.3g/day of sodium.
- Avoid foods high in sodium and fat (trans and saturated fat) Consume feeds rich in calcium and magnesium.
- monitor for hyperkalemia with salt substitute use.
Medications: Table 31-4
- Diuretics: Thiazide diuretics inhibit water and sodium reabsorption and increase potassium excretion.
- Other diuretics can treat hypertension that is not responsive to thiazide diuretics such as loop diuretics and potassium diuretics.
- Monitor potassium levels and watch for muscle weakness, irregular pulse, and dehydration.
- Thiazide and loop can cause hypokalemia, and potassium-sparing diuretics can cause hyperkalemia.
- Ace inhibitors: (end in -pril) prevents the conversion of angiotensin I to angiotensin II, which prevents vasoconstriction.
- Hypotension is a common adverse effect.
- Monitor for evidence of heart failure, edema.
- ACE inhibitors can cause heart and kidney complications.
- Teach the client to report a cough as it’s an adverse effect.
- Beta blockers: (end in -olol) for clients with unstable angina and MI.
- They decrease cardiac output and block the release of renin, decreasing vasoconstriction of the peripheral vasculature.
- These meds can mask hypoglycemia in clients with DM.
- Other diuretics can treat hypertension that is not responsive to thiazide diuretics such as loop diuretics and potassium diuretics.
What does the medications do for the patient? How does the nurse know the medications are working? Side effects? What needs to be monitored?
- The patients bp should be lower than 140/90.
- When the patient returns for follow up care, all body systems must be assessed to detect any evidence of vascular damage.
- An eye examination with an ophthalmoscope is important to detect retinal blood vessel damaged which indication similar damage elsewhere in the vascular system.
- The patient is questioned about blurred vision, spots in the front of eyes and diminished visual acuity.
- The heart, nervous system, and kidneys are assessed.
- The patient should report no changes in vision, edema, dyspnea, no motor, sensory, or speech deficits.
- Urine output should be consistent with input, no headaches, weakness, or falls. Any significant findings may indicate the need to change medications and additional diagnostic tests may be needed such as urinalysis, blood chemistry, a 12-lead electrocardiogram, and echocardiography.
- Additional studies, such as creatinine clearance, renin level, urine tests, and 24-hour urine protein.
- When the patient returns for follow up care, all body systems must be assessed to detect any evidence of vascular damage.
Diabetes:
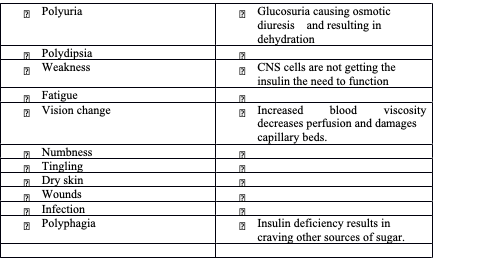
1. Describe the clinical manifestations of persons with diabetes. General Signs and Symptoms of Diabetes
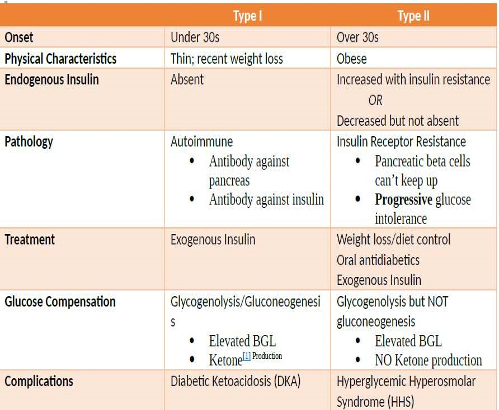
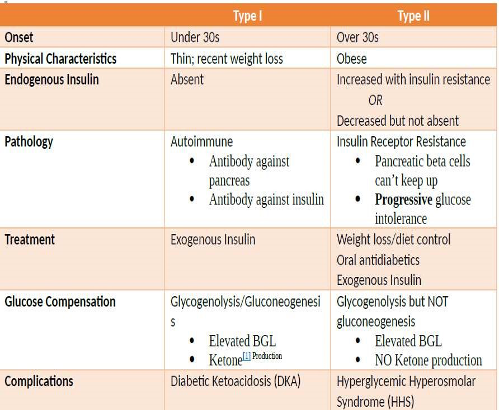
Type I vs Type II Diabetes
Criteria for Diagnosing Diabetes
*note – PGL plasma glucose level {there is a difference between a PGL and a BLG (blood glucose level).
The textbook talks about obtaining plasma glucose levels.
- Ketones – a highly acidic substance formed when the liver breaks down free fatty acids in the absence of insulin
- Classic Signs of Diabetes – Polyuria, polydipsia, and weight loss
2.Explain the relationship between diabetes and other disease processes Macrovascular disease – usually associated with type II diabetes.
- Pathology – Increased atherosclerosis [1] leading to ischemia
- Changes in arterial walls r/t hyperglycemia and hyperinsulinemia Changes in platelet and clotting factors Decrease in RBC flexibility.
- Decrease in oxygen release. Specific Processes
- Coronary Artery Disease (CAD)
- MIs are more likely to occur, reoccur, and cause death.
- MIs may not have ischemic signs and symptoms silent MI related to neuropathy.
- Cerebrovascular Disease
- Thrombus of cerebral vessel or emboli that lodges in cerebral vessel Recovery is also hampered in diabetics.
- HHS and DKA symptoms may be similar to those of a stroke. Peripheral Artery Disease (PAD)
- S&S diminished peripheral pulses, claudication, pale skin
- PAD can progress resulting in ischemia, gangrene and need for
- amputation
- Microvascular – usually associated with type I diabetes.
- Pathology
- Elevated glucose causes a thickened capillary basement membrane.
- Specific Processes
- Diabetic Retinopathy
- Leading cause of blindness in ages 20-74
- Microvascular changes of retinal [2] blood vessels cause.
S&S of Retinopathy
- Many are asymptomatic until proliferative stage.
- Floaters/cobwebs
- Sudden, spotty, hazy vision
- Sudden complete loss of vision
Diabetic Nephropathy
- Microvascular changes to and around kidney filtration mechanism
- Caused by osmotic pressure placed on kidneys by excreted glucose and protein
- Damage to kidneys can increase BP.
Neuropathic – nerve damage caused by chronically elevated BGL.
Pathology
- Thickening and closing of capillary membrane around nerves decreases nerve. perfusion
- Demyelization of nerves slows/disrupts nerve conduction.
Specific Processes
- Peripheral (sensorimotor) polyneuropathy
- Paresthesia
- Decreased proprioception.
- Charcot joints [3].
- Decreased deep tendon reflex.
- Autonomic neuropathy affects every organ of the body. Cardiovascular Neuropathy Fixed, tachycardic HR.
- Orthostatic hypotension
- Silent MI Gastrointestinal Neuropathy Delay gastric emptying.
- Constipation or diarrhea
- Wide swings in BGL due to inconsistent GI absorption of glucose
- Renal/Bladder Neuropathy
- Urinary retention with decreased sensation of fullness
- UTIs
Adrenal Medulla Neuropathy
- Hypoglycemic unawareness
- Adrenal glands no longer respond to hypoglycemic conditions.
Sudomotor Neuropathy anhidrosis (absent sweating) related to diabetic neuropathy.
- Sexual Dysfunction Reduced vaginal lubrication. Decreased libido.
- Vaginal infections
- Erectile dysfunction/retrograde ejaculation Cranial mononeuropathies
Others
Hypertension – most common complication in people with diabetes but may not bedirectly caused by diabetes.
- High cholesterol = HTN
- Kidney damage = HTN
- Vascular damage = HTN
- Erectile dysfunction = HTN related medications
Metabolic Syndrome interrelated conditions typical of type II diabetes
- Atherosclerosis – blood vessel wall thickening, sclerosing, and becoming occluded by plaque.
- Retina – the part of the eye that receives and sends images.
- Charcot Joints – neuropathy related joint changes, often found in the foot, caused by abnormal weight distribution.
- Explain the psychological and sociological effects of diabetes in the individual and family.
Implementing nutritional changes can affect the entire family.
- Hypoglycemia/DKA/HHS can be traumatic experiences for the family.
- Children with diabetes have a significant impact on their family.
- Administering injections
- Sudden blindness caused by diabetes can be the first indication of diabetes.
- Compare and contrast the pharmacological management and nursing implicationsassociated with people with diabetes.
- General Nursing Considerations Monitor BGL
- Beta-blockers may block S&S of hypoglycemia.
Ultra long acting insulin provides additional glucose control and lasts for more than 24 hrs
[1] Lactic Acidosis S&S – myalgia, sluggishness, somnolence, hyperventilation
- Apply the concepts of nutrition to the care of persons with diabetes
- Nutrition, meal planning, weight control, and increased activity are the foundation of diabetes management.
- Control total caloric intake to attain or maintain a reasonable body weight,
- Control of blood glucose levels, and normalization of lipids and blood pressure to prevent heart disease.
- Registered dietician and RNs responsible for design and educate about aspects of a therapeutic plan.
- A meal plan for diabetes focuses on the percentages of calories that come from carbohydrates, proteins, and fats. OH=risk for hypoglycemia.
- Appraise the learning needs and develop teaching plans for the person with diabetes.
- Nursing management of patients with diabetes can involve treatment of a wide variety of physiologic disorders, depending on the patient’s health status and whether the patient is newly diagnosed or seeking care for an unrelated health problem. Monitor glc levels, Assess self-care skills.
- Provide basic education.
- Reinforce the education provided by the specialist and refer patients for follow-up care.
- Nursing management of patients with diabetes can involve treatment of a wide variety of physiologic disorders, depending on the patient’s health status and whether the patient is newly diagnosed or seeking care for an unrelated health problem. Monitor glc levels, Assess self-care skills.
- Identify the nursing responsibility in the short and long-term management (including discharge instructions) of the person with diabetes.
- Teachpt about diet = limit carbs, increase protein, limit fats, medication, exercise @ least 3X/wk, sleep, encourage weight loss, self-management skills, monitor blood glc and prevent complications.
- Teach pt and family members S&S of hypo and hyperglycemia.
- Diabetes management has five components:
- Teachpt about diet = limit carbs, increase protein, limit fats, medication, exercise @ least 3X/wk, sleep, encourage weight loss, self-management skills, monitor blood glc and prevent complications.
nutritional therapy, exercise, monitoring, pharmacologic therapy, and education.
Need to do constant assessment.
o Diabetes
- Type I and II Diabetes ( know the differences)
- Clinical Manifestations – hypoglycemia & hyperglycemia
Note: Additional info below if you want to go over it, if not continue part C. Nutrition Hypoglycemia- < 65, devastating effects on the CNS b/c relies on glc for energy if no glc lead to cell death.
*How can it happen?
- Too much insulin circulating, overly high dose of oral hypoglycemic.
- Reduced clearance of insulin from the body because of renal insufficiency *Who is at risk?
- Decreased nutritional intake.
- Increase metabolism d/t exercise.
- Alcohol can reduce glucose levels too by blunting the release of glucose from the liver.
- Can be more severe if the early signs are blunted – pt. isn’t aware – one thing you might see is a change in mental status in the elderly.
*S&S
Anxiety, palpitations, hunger, paresthesia (numbness at lip), sweating, shakiness.
*If it continues to drop – where the CNs would be involved
- Difficulty thinking, dizzy, fatigue, sleepiness, slurred speech, weakness lack of coordination.
*If continues to be untreated: seizures coma
If a patient suffers from hypogly frequently – they may be unaware of early symptoms – this patient should increase their BS control number to avoid hypogly events.
Hyperglycemia = Diabetic Ketoacidosis (DKA) BG > 250
*Causes – missed dose of insulin /inadequate insulin d/t increases insulin needs secondary to stress or infection
New dx of DM 1 *How is it diagnosed?
- ketones in the urine
- arterial pH <7.30
- serum bicarb <15
- Positive anion gap
*S&S
The three P’s.
- Pt. becomes dehydrated- electrolyte imbalance. Increase or decrease K+ Fluid shift from intracellular to the extracellular.
- Leads to dilution AL hyponatremia.
- Patient at risk/f hypovolemia 2’ to the osmotic diuresis.
*If not treated what happens?
- Hypotension, tachycardia secondary fluid vol. loss.
- Kussmaul respiration develop – these are rapid deep respirations this is a compensatory mechanism for acidosis.
- fruity acetone breath – because of the ketone bodies s
- n/v
- lethargy, coma *Treatment
- Fluid replacement – NS (isotonic)
- Insulin administration
- Correction of electrolyte imbalance.
C. Nutrition – timing of snacks when giving insulin, general diet teaching
- If a patient is in Lispro (rapid acting insulin) give it w/food bc it works quickly. Highest risk
- for hypoglycemia is when it reaches peak level so here is when you need a snack for
- the patient. Know peak time=snack time
- N 3561 Exam 1 Exam Blueprint
- Diabetic diet = limiting carbs or counting carbs. Pt edu @ bedside but need support when they go home they need to consult a dietician to help them with diet at home. D. Acute and chronic complications: DKA, HHNS, hypoglycemia , effects on organs.
- *DKA
- hypotensive tachy secondary vol. loss.
- kussmauls respirations develop – these are rapid deep respirations this is a
compensatory mechanism for acidosis. fruity acetone breath – because of the ketone bodies n/v
- lethargy
- Coma
*HHNS-Hyperosmolar Hyperglycemic Non-Ketosis or Hyperglycemic
- Hyperosmolar State (HHS) is serious event, glucose levels rise toward 600 +
- Characterized by hyperglycemia hyperosmolarity and dehydration without ketoacidosis (big distinguishing factor)
- *It occurs when there is sufficient insulin to prevent the breakdown of fat and ketone release BUT not enough insulin to prevent severe hyperglycemia
- *Because of this the body compensates this leads to extreme hyperosmolarity leads to osmotic diuresis –
- The patient became severely dehydrated!!!! And suffers from electrolyte.
- imbalances (severe)
- They may also present with neuro defects.
- *It is less common then DKA
- Does have a higher mortality rate than DKA. Hypoglycemia
- *If insulin continues to drop – the CNs would be involved
- Difficulty thinking, dizzy, fatigue, sleepiness, slurred speech, weakness lack of coordination.
- *If continues to be untreated: seizures coma
- If a patient suffers from hypoglycemia frequently – they may be unaware of early symptoms – this patient should increase their BS control number to avoid hypoglycemia event.
What are the long-term effects of DM on organs?
- The immune system can be impacted – this can lead to infection and poor wound healing, foot ulcers,
- Puts patients at risk for longer hospital stays – sepsis – tissue damage Vascular effects & heart failure.
- Can be macrovascular (large arteries ) and microvascular ( small bld vessels)
- Eyes (Retinopathy)
- Gums (Periodontal)
- Kidneys (Nephropathy)
- PVD & PAD
- Neurological effect
- Diabetic peripheral neuropathy
- Autonomic neuropathy – gastropareses (pt eats and stomach doesn’t empty or nauseous) ED orthostatic hypertension.
- Urinary problems – difficulty starting stream.
- inability to empty bladder completely
- leads to UTI,
- Cardiovascular disease – most likely will have some sort of cardio problem.
- 75% higher risk for blockage.
- fertility issues, liver dz, amputations
Sick day management. Exercise management,
*Sick day management keep monitoring blood glucose because blood sugar can go up. Illness or stress can trigger hyperglycemia. If a diabetic pt is admitted to hosp. and A1C is high find out why maybe underlying infection.
- *Exercise at the same time of day (preferably when blood glucose levels are at their peak) and for the same duration each session. Inspect your feet daily after exercise.
- Avoid exercise in extreme heat or cold. Avoid exercise during periods of poor metabolic control.
- Eat a snack at the end of the exercise session and at bedtime and monitor the blood glucose level more frequently.
- Know the insulins – onset, peak and duration, metformin too, Know the insulins – onset, peak and duration, metformin too. Onset Peak Duration
- *Rapid acting lispro – 10–15 minutes 1 hours 2-4 hrs.
- Used for rapid reduction of glucose level, to treat postprandial hyperglycemia, and/or to prevent nocturnal hypoglycemia.
- *Short acting regular (Humulin R, Novolin) 30–60 minutes 2–3 hours 4–6 hours given 20–30 minutes before a meal.
- alone or w/long acting
- *Intermediate acting: NPH (neutral protamine Hagedorn) 2–4 hours 4–12 hours 16–20 hours taken after food.
- *Very long acting: glargine (Lantus) detemir (Levemir) glargine 1-6 hrs. (no peak, cont.) 24 hrs. or 24–36hrs Used for basal dose.
* Metformin oral antidiabetic.
- Inhibit production of glc by the liver. start pt @ lower dose possible and then gradually increase it.
- Med will work to decrease the amount of
- circulating glc. Need to monitor blood glc and take it every day. Can be used in comb w/insulin or other antidiabetic agents.
- *Extra info!
- *Pts on metformin discontinue the oral agent 24 to 48 hours before surgery, if glc not well controlled with diet and an oral antidiabetic agent before surgery) need to continue with insulin injections after discharge.
- *Pt with minor surgery and stable glc level no dextrose is infused during the surgery.
- After surgery, these patients may require small doses of regular insulin until the usual diet and oral agent are resumed.
- *Metformin should be stopped 48 hours prior to and for 48 hours after the use of contrast agent or until kidney function is evaluated and normal.
*NOTE: prof said peak onset and duration commit to memory!
- The primary goal of treatment to maximize glycemic control for both type 1 and 2.
- Achieve normal glc levels (euglycemia) without hypoglycemia while maintaining a high quality of life.
Sick day management
If pt sick they should increase their blood sugar checks What can increase blood sugar?
If conscious: oral glucose administration, can give any form of a carbohydrate like juice soda, bread, or crackers.
- Carbs that contain fat are not recommended – like ice cream.
- Once taken recheck BS in 15 mins.
- If unable to swallow – and has IV access- give D50 25-50 ml.
- If no IV access- 1mg IM glucagon
- Teach family members about the symptoms and how to treat them.
- Check blood sugar levels 15 minutes after treatment.
Effect of exercise – education needed.
- *Exercise 3X wk.
- teach pt that blood sugar will decrease so they need to know how to respond,
- Check blood sugar before exercise, and if exercising for a long period of time check blood sugar before and after. If heavy exercise (check during).
- They should have candy & eat it if hypoglycemia symptoms.
- If using insulin, abdomen is best bc better absorption rate.
- *Increased blood pressure associated with exercise may aggravate diabetic retinopathy and increase the risk of a hemorrhage into the vitreous or retina.
Practice questions
- The nurse is reviewing laboratory values and notes that a patient will soon begin treatment for diabetes mellitus. Which glycosylated hemoglobin (A1C) level is on the patient’s medical record?
- A.1.7%
- B.3.4%
- C.5.2%
- D.6.8%
- C.6.8%
Rationale:
According to the American Diabetic Association diagnostic criteria, a hemoglobin A1C greater than or equal to 6.5% support the diagnosis of diabetes mellitus.
- The nurse correlates which laboratory values as a diagnostic for DKA? Select all that apply.
- A. serum bicarbonate of 15
- B. negative anion gap
- C. serum glucose of 350
- D. positive anion gap
- E. arterial pH of 7.36
- C, d
- The nurse is preparing to instruct a patient with type 1 diabetes mellitus on the complication of diabetic ketoacidosis. Which pathologic process should the nurse review with the patient about this complication?
- A.A decreased amount of glucagon causes low protein levels
- B. An excess amount of insulin drives all glucose into the cells
- C. A deficit of insulin causes fat stores to be used as an energy source
- D.An increase occurs in the breakdown of glucose molecules with hypoglycemia
- C.A deficit of insulin causes fat stores to be used as an energy source
Rationale: Untreated the glucose deficit in the cells causes fat store to break down to provide energy…..increased ketones….ketones are acids….causes metabolic acidosis DKA = Metabolic Acidosis
- The nurse is providing discharge instructions to a patient with type 2 diabetes mellitus.
Which patient statement indicates teaching about foot care at home has been successful?
- A. “I always buy my shoes as soon as the stores open
- B. “I will walk barefooted as long as I am in the house”
- C. “I will check my feet for cuts and bruises every night”
- D. “If I get a blister, I will just put alcohol on it and bandage it
- C . “I will check my feet for cuts and bruises every night”
Rationale: Visual inspection of the feet each day in important in preventing more serious complications. Shoes should be purchased later in the day when feet are at their largest. Footwear should always be worn. The patient should be instructed to never walk barefoot. Foot wounds should be treated by a healthcare professional.
- 5. The nurse identifies the nursing diagnosis RISK FOR INJURY as appropriate for a patient with type 2 diabetes mellitus because of peripheral neuropathy involving both feet. Which assessment would support this diagnosis?
- A.Loss of normal reflexes
- B.Normal sensation to touch
- C.States “I can’t feel my feet anymore”
- D.States “I have been having chest pain”
- C.States “I can’t feel my feet anymore”
- A.Loss of normal reflexes
- Rationale: Diabetics are at risk for injury due to multiple factors. Neuropathies alter sensation, gait, and muscle control. There is an increased risk of accidents, burns, falls, and trauma.
Vascular Problems:
Vascular Problems: (Kim R)
The 6 P’s to Assess Arterial Occlusion:
- Pain
- Pallor
- Pulselessness
- Paralysis
- Paresthesia
- Poikilothermic – decreased temp. in leg Vascular Problems
- Compare & contrast signs & symptoms of arterial vs. venous – (be able to recognize thedifference )- disorders.
- Discuss the role of common risk factors associated with the of atherosclerosis.
- Atherosclerosis – plaque buildup in artery walls. Plaque is fat deposits, cholesterol, and other substances = decreased blood flow.
- If it becomes brittle or inflamed, it ruptures and causes blood clot = increased blockage of arteries.
- Peripheral Arterial Disease (PAD) is usually caused by atherosclerosis. Atherosclerosis can cause artery narrowing (stenosis), obstruction via thrombosis, aneurysm, ulceration, and ruptures.
- Risk factors:
- Modifiable Risk Factors: Tobacco use
- Diets high in fat
- Hypertension
- Diabetes
- Hyperlipidemia
- Stress
- Sedentary lifestyle
- Elevated C-reactive protein
- Hyperhomocysteinemia (abnormally high level of homocysteine in the blood, conventionally
- described as above 15 μmol/L.
- As a consequence of the biochemical reactions in which homocysteine is involved, deficiencies of vitamin B , folic acid, and vitamin B can lead ₆₁₂ to high homocysteine levels) Nonmodifiable Risk Factors:
- Increased age
- Female gender
- Family predisposition/genetics.
- Atherosclerosis – plaque buildup in artery walls. Plaque is fat deposits, cholesterol, and other substances = decreased blood flow.
- Discuss medical, surgical, and nursing management of venous & arterial disorders.
ARTERIAL DISORDERS
- Arterial disorders include atherosclerosis, PAD, Upper extremity arterial occlusion disease, aortoiliac disease, aneurysms, dissecting aorta, and arterial embolisms/thrombosis.
- PAD: commonly found in femoral-popliteal and below the knee in diabetics
- Medical: Treated with
- exercise like walking and arm-ergometer exercises to decrease pain associated with claudication.
- Vasodilators, Antiplatelets: aspirin and clopidogrel, and statins used.
- Surgical:
- Stent in artery to hold it open,
- Endarterectomy – removal of plaque, Arterial Bypass, and Grafts (high complication rate postop).
- Nursing:
- exercise like walking and arm-ergometer exercises to decrease pain associated with claudication.
lower legs below heart (neutral or dependent position), encourage walking/moderate exercise.
- Upper Extremity Occlusion Disease: less common and less severe. Usually result from trauma or atherosclerosis.
- Medical: stents, bypass, grafts.
- Nursing: BP in both arms, use of doppler flow if pulses hard to find. Same signs as in legs.
- Aortoiliac Disease:
- stenosis or occlusion in aorta causes butt and lower back pain, or impotence in men.
- Surgery is necessary to fix.
- Assess all pulse placements in arms and legs, I&Os, and abdominalsounds.
- stenosis or occlusion in aorta causes butt and lower back pain, or impotence in men.
- Aneurysms:
- The sac dilated off weak point in an artery.
- Thoracic aneurysms are most common and caused by atherosclerosis. Requires surgery and post-op care.
- Dissecting Aorta: tear in aorta; more common in men. Causes chest pain that shoots to shoulder and mistaken as MI.
- Arterial embolism and thrombosis: Acute occlusion of emboli mainly develop from thrombi in the heart from Afib/MI/CHF.
- 6 P’s associated with acute occlusion.
- The sac dilated off weak point in an artery.
- Medical: Heparin therapy immediately! thrombolytics
- Surgical: Embolectomy and thrombectomy
- Nursing: bed rest before surgery, protect affected area, anticoagulation therapy, and start walking after surgery. Assess pulse, Doppler, and ABI.
- Medical: stents, bypass, grafts.
VENOUS DISORDERS
- Venous disorders include DVT, PE, chronic insufficiency/Post thrombotic syndrome, leg ulcers, varicose veins.
- DVT and PE are clinically silent.
- DVT: unilateral thrombosis frequently accompanied by phlebitis.
- Virchow’s Triad: 3 main risk factors leading to DVT are 1. Stasis, 2. Hyper coagulability, and 3. Vessel Wall Injury.
- Edema, swelling, tenderness, warmth, feeling of heaviness in legs.
- Medical: Anticoagulation therapy (prevents new thrombus formation NOT dissolve already formed thrombus), thrombolytics.
- Nursing: monitor bleeding, elevate leg above heart, compression stockings, walking once anticoagulation therapy starts, bed exercises
- Venous insufficiency from obstruction or blood reflux of valves.
Post thrombotic syndrome: chronic stasis, edema, pain, and dermatitis.
- Nursing: Elevate legs, graduated compression stockings, sleep with feet elevated, walking, keep skin clean and dry.
Venous ulcers – more common than PAD ulcers.
- Occur at media land lateral malleolus, large, superficial, exudative aka WET ULCER.
- Nursing: Debridement of ulcer, wound dressings, negative pressure wound therapy, hyperoxygenation.
Varicose Veins: bad valves cause backflow of blood to outer, superficial veins.
- Causes pain, dull ache, feeling of fullness, ankle edema.
- Surgical:
- vein stripping if needed but usually not necessary.
- Sclerotherapy helps but does not cure them.
- vein stripping if needed but usually not necessary.
- Nursing: elevate legs, change positions often, avoid restrictive clothes.
- Surgical:
Remember severity of pain NOT related to size of varicosities.
- Develop a teaching plan for a patient with arterial/venous occlusive diseases. Discourage tobacco use.
- Keep warm temperature to prevent vasoconstriction.
- Manage stress.
- Proper clothes that are not restrictive/tight = decreased blood flow and venous stasis.
- Take meds as prescribed.
- Promote exercise to increase circulation.
- Protect skin and extremities from trauma because of delayed wound healing.
- Wear protective shoes and pad pressure areas. Inspect feet and legs often.
- Encourage meticulous hygiene.
- Promote good nutrition for wound healing – Increase protein intake, vitamin A and C, and Zinc.
- Include family in teaching, provide written material, and refer to resources such as exercise groups or support groups for smoking cessation.
- Describe complications of peripheral vascular disorders and measures to prevent theiroccurrence.
- Bleeds from heparin
- Thrombosis, PE
- Contraindications to peripheral thrombolytic therapy include active internal bleeding, cerebrovascular hemorrhage, recent major surgery, uncontrolled hypertension, and pregnancy.
- Cellulitis, dermatitis, and ulceration from venous insufficiency
- Identify & describe nursing intervention priorities for patient with vascular problemsincluding cellulitis.
Cellulitis:
- Common infection caused by limb swelling by allowing bacteria to enter subcutaneous skin layer.
- Signs of swelling, localized redness, warmth, and pain accompanied with fever/chills/sweating.
- Pitting “orange peel” appearance. Interventions
- Elevate affected area 3-6 inches above heart level, apply cool/moist packs to site every 2 hours to resolve inflammation, then finish with a warm pack.
- Caution with warm packs in patients with decreased sensory of temperature like diabetics (could cause burns).
Thrombophlebitis – heparin, coumadin (warfarin), Lovenox – teaching involved, labs to monitor, signs of complications.
- Prevention of clots:
- Lovenox as prophylactic Ambulate
- sequential stockings/hose.
- If clot developed, Heparin (anticoagulant) is used to prevent further clotting. (SubQ). Monitor aPTT for dose adjustment.
- If aPTT goes too HIGH = too much thinning blood = Give protamine sulfate(Vitamin K).
- Monitor platelet count because it can cause issues with them. Should be greater than 100,000 platelets.
- Monitor for bleeding (nose bleeds, bruises, gums)
- Enoxaparin (Lovenox) given SubQ as prophylaxis and treatment of VTE.
- Air bubbles at end DON’T push out.
- Fewer bleeding complications than heparin.
- Less monitoring required. Just platelet count.
- After heparin and Lovenox use in hospital and going home, put on either Coumadin (Warfarin) or Xarelto.
- Coumadin – Oral anticoagulant helps get up to therapeutic range so given with Heparin near the end of hospital stay.
- Coumadin use PT and INR to monitor. Want above the “normal” range.
- Xarelto – no antidote, caution. Expensive!
- Meds that decrease clot formation & treat PAD:
- Lovenox – Antithrombo.
- Aspirin – thins blood
- Plavix – antiplatelet
- Pletal – anticoagulant
- Trental – anticoagulant
Raynaud’s disease (what is it , who is at risk , what do they need to avoid)
- A form of intermittent arterial vasoconstriction of the fingertips and toes = coldness, pain, tingling, numbness, and pallor.
- Primary Raynaud’s: occurs in absence of an underlying disease.
- Secondary Raynaud’s: (Syndrome) Associated with underlying diseases like lupus, rheumatoid arthritis, scleroderma (common), trauma, or obstructive arterial lesions.
- Triggered by stress and cold conditions.
- Very common in women.
- Medical management: avoid smoking and the cold.
- Calcium channel blockers can relieve symptoms.
- Nursing management: Avoid stressful situations, wear warm layers in cold, stop smoking.
- Uncommon complications – gangrene and amputation.
- Postural hypotension as an adverse effect of calcium channel blocker medications.
For all of the above topics , recognize risk factors, symptoms, management both medical and nursing, treatment – know medication if it is indicated for diagnosis –