Understanding emr and ehr: A Nursing Student’s Guide to Electronic Health Records
In modern clinical environments, nursing students step into settings where documentation is no longer confined to binders and filing cabinets, but instead lives within complex digital systems that shape every aspect of patient care. The ability to navigate an emr or an electronic health record is now as foundational as mastering vital signs or conducting a physical assessment. Far from being simple charting platforms, these systems represent the evolving structure of clinical communication, continuity of care, and decision-making across disciplines.
Understanding what an electronic medical record is—and, more importantly, how it functions within real clinical workflows—allows nursing students to appreciate how digital documentation supports safe practice. These systems consolidate assessments, medications, progress notes, diagnostic results, and other forms of health information that guide clinicians’ daily interactions with patients. Because the shift from paper to digital documentation has transformed how nurses assess, record, and retrieve details about a patient’s condition, nursing students benefit from recognizing how these tools influence both individual responsibilities and collaborative care.
Conversations around ehr vs emr are not merely technical distinctions; they highlight critical differences in scope, accessibility, and the sharing of patient data across departments and care settings. For students entering clinical rotations, understanding how these digital systems are designed, what they store, and how nurses use them in real time is essential to delivering thorough, accurate, and legally sound documentation. Digital charting supports the clinical reasoning process, helps detect changes in patient status more efficiently, and strengthens communication among interdisciplinary teams.
Just as nursing students learn to interpret trends in patient assessments, they must also learn to interpret and navigate the digital environments where those assessments live. Becoming fluent in the language and logic of electronic documentation helps students feel more confident, reduces errors, and prepares them to engage thoughtfully with the technology that underpins modern healthcare practice. This guide provides a structured, comprehensive exploration of EMR and EHR concepts, practical documentation skills, and the implications these systems have on patient care and professional competence—ensuring that nursing students are well-equipped to chart effectively, think critically, and participate fully in today’s digitally integrated clinical settings.
What is an electronic medical record (emr) and how is it used?
An emr system is the digital foundation of clinical documentation within a single healthcare facility, functioning as a centralized platform that stores and organizes information essential for day-to-day care. It contains a patient’s medical history, treatment plans, medication lists, allergies, and diagnostic results, making it easier for nurses and providers to access the information they need to make informed clinical decisions. Designed to replace paper records, the EMR provides a safer, more consistent method of capturing ongoing care, reducing documentation errors and improving workflow efficiency in settings such as primary care clinics, inpatient units, and specialty practices.
Because EMRs collect extensive clinical data, they become the primary source of truth for understanding trends in a patient’s health over time. For instance, when a nurse measures vital signs at the bedside, the information is recorded immediately, time-stamped, and added to the evolving record of a patient’s health. These digital entries help ensure that assessments remain accurate, up to date, and available to all members of the care team who need them.
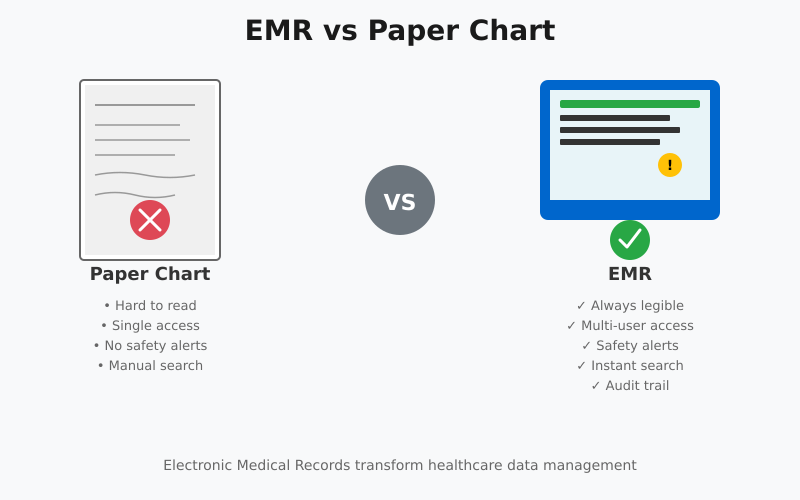
What is an emr and how does it compare to a paper chart?
- Legibility, speed, and access. Unlike paper records, EMRs are searchable, legible, and can be accessed simultaneously by multiple authorized users (rather than a single person rifling through paper files). These features speed retrieval of medication lists, recent labs, and prior notes—advantages repeatedly reported in implementation studies.
- Structured fields vs. free text. Paper charts often rely on narrative notes and scanned documents. EMRs combine structured data fields (medication lists, problem lists, coding fields) with sections for free-text notes; this structure makes data available for analytics, reminders, and quality measurement in ways paper charts cannot.
- Auditability and safety features. EMRs keep an audit trail (who entered or edited what and when), time-stamped entries, and safety alerts (for allergies or drug interactions). Paper records lack these automatic safety and accountability features.
How does an emr system store medical history and clinical data?
EMR systems store information in a mixture of structured and unstructured formats:
- Structured data are discrete, coded elements (e.g., demographics, medication start/stop with timestamps, vital signs, lab values, ICD/diagnosis or SNOMED codes). These fields are ideal for trend displays, clinical decision support (CDS) and reporting.
- Unstructured data include narrative progress notes, free-text social history, and scanned documents. While rich in clinical detail, unstructured text is harder to query programmatically and requires natural language processing or manual review to extract discrete data.
- Attachments and multimedia. EMRs can link or store images (wound photos, radiology reports), PDFs (consult letters), and other artifacts that previously would have been paper inserts. All items are indexed to the patient’s record and are retrievable by date and encounter.
A practical storage example: a primary-care visit entry might include discrete vitals (height/weight/BP), a coded diagnosis of “hypertension,” a structured list of current medications, and a narrative note describing the patient’s symptoms and plan. The vitals and medication list can automatically feed into flow sheets and trend graphs; the narrative explains contextual details clinicians need for decision-making.
How do clinicians use emrs for diagnoses and patient data entry?
- Problem lists and diagnostic coding. Clinicians add diagnoses to a problem list so subsequent users see the working problems for that patient; this list supports encounter documentation, billing, and quality reporting. Correct and timely updating of the problem list reduces ambiguity in care planning.
- Order entry and documentation at point of care. Providers place electronic orders for labs, imaging, and medications directly in the record (Computerized Provider Order Entry), reducing transcription errors and enabling electronic tracking of results. Nursing documentation (e.g., medication administration records, flow sheets) is entered in structured modules or encounter notes to reflect care provided in real time.
- Clinical decision support (CDS). Many EMRs include CDS: alerts for drug interactions or allergies, reminders for preventive care, and evidence-based suggestions (e.g., recommended antibiotic choice). These tools are embedded at the point of documentation and can influence diagnostic reasoning and treatment choices.
Example scenario for nursing students
Imagine a patient with hypertension seen across three visits: on each encounter, the nurse records vitals into the EMR’s discrete fields; the system graphs blood pressure over time. The provider updates the problem list with “essential hypertension” (a coded diagnosis). A CDS reminder flags that the patient is overdue for renal function testing before starting a new antihypertensive—prompting an order placed through the EMR. The nurse later documents the lab draw and medication education in the encounter note. Compared with a paper chart, this electronic workflow preserves discrete data for trends, triggers safety checks automatically, and keeps all team members informed in near real time.
How does an electronic health record (ehrs) differ from an emr?
Understanding the differences in the ehr vs emr discussion is essential for nursing students because these systems directly influence documentation, patient safety, communication, and workflow efficiency. Although the terms are often used interchangeably in clinical settings, an emr and an EHR operate on different scales and serve different purposes within healthcare.
An emr (electronic medical record) is essentially a digital version of a patient’s chart within a single healthcare practice. It includes clinical data such as diagnoses, medication lists, laboratory results, and progress notes documented by the providers in that specific practice. For example, a family medicine clinic may use an emr to track a patient’s hypertension treatment plan, manage follow-up appointments, and record medication refills. However, this information typically cannot be easily shared outside that clinic unless exported manually. This is one of the biggest distinctions highlighted in the ehr vs comparison.
In contrast, an electronic health record (EHR) is designed for interoperability, meaning it is built to be shared across multiple healthcare providers and organizations. In the ehr vs emr comparison, an EHR contains everything an EMR does plus additional features that support integrated, longitudinal care. An EHR follows the patient across settings—primary care, specialty clinics, emergency departments, rehabilitation centers, and even long-term care facilities. A nursing student working in a busy hospital ward, for example, benefits from having access to the patient’s EHR, which may include their outpatient cardiology notes, previous imaging, chronic disease management data, and up-to-date medication reconciliation.
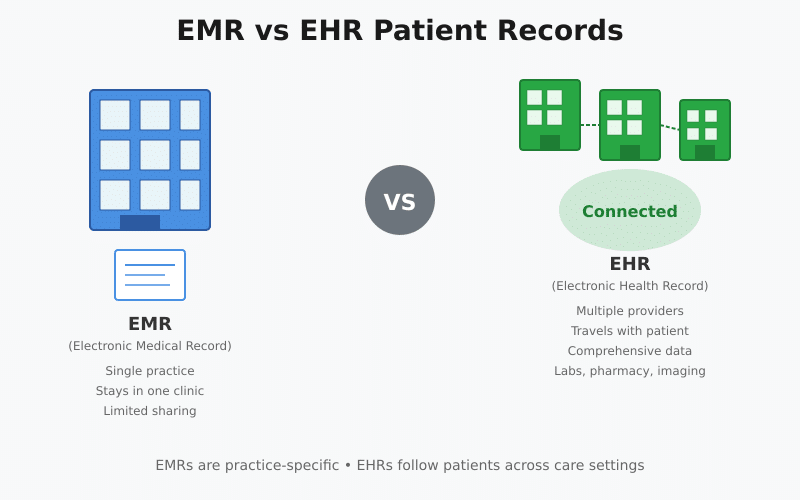
What’s the difference between an emr and an ehr in patient records?
The ehr vs emr difference becomes clear when examining how patient records are structured and used.
EMR patient records:
- Are practice- or organization-specific
- Serve as a legal, clinical record for one clinic
- Support diagnosis, treatment, and charting within that environment
- Usually do not travel with the patient without special transfer processes
EHR patient records:
- Are comprehensive, multi-source health profiles
- Follow the patient across multiple care settings
- Support population health, quality improvement, and patient safety
- Integrate data from pharmacies, labs, imaging centers, and specialists
For example, if a patient with diabetes is referred from a primary care clinic (using an emr) to an endocrinologist, the new provider may not automatically see the full record unless the nurse or clinic staff prints or electronically sends the information. With an EHR, however, the endocrinologist, primary care provider, and nurse navigator can all view the same updated record in real time.
How do ehrs support care coordination across healthcare providers and organizations?
One of the strongest arguments in the ehr vs emr discussion relates to care coordination. EHRs are specifically designed to enhance communication and continuity of care. They make it possible for healthcare teams to:
- Share test results, diagnoses, and treatment plans instantly
- Prevent duplicate tests or conflicting medications
- Reduce medical errors and improve patient safety
- Communicate between inpatient and outpatient care teams
For instance, when a patient is discharged from a hospital, an integrated EHR automatically updates the primary care provider with discharge summaries, new prescriptions, and follow-up needs. Nurses in outpatient settings benefit by reviewing these updates before the patient’s next appointment, ensuring continuity and avoiding care gaps.
By contrast, an emr does not naturally support this type of coordination because it is isolated within one organization. This limitation is central to the ehr vs debate when planning system-wide improvements in healthcare delivery.
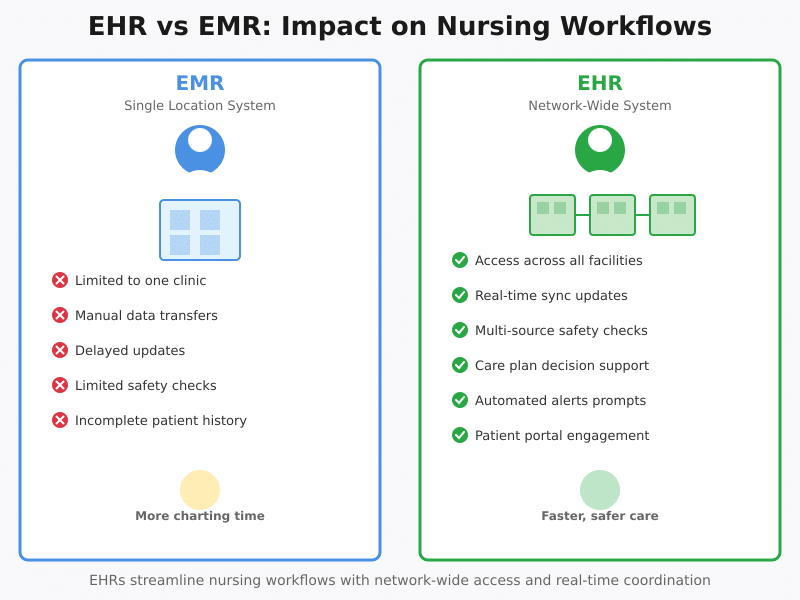
Which key differences between ehr and emr affect nursing workflows?
Nursing workflows depend heavily on efficient, accessible patient information. Several key differences in the ehr vs emr comparison directly influence how nurses deliver care:
1. Accessibility Across Care Settings
- EHR: Nurses can access patient data anywhere within the health network—ER, ICU, outpatient clinic, or rehab facility.
- EMR: Access is limited to one location or organization.
Example: A nursing student doing clinicals in a hospital can quickly pull up a patient’s EHR showing lab results from an outside facility. With an emr, this information may not be available unless uploaded manually.
2. Real-Time Updates
- EHR systems synchronize updates instantly across teams, supporting better handoffs and interdisciplinary communication.
- With an emr, delays can occur if data needs to be transferred or re-entered.
3. Medication Safety and Reconciliation
EHRs automatically check interactions using data from multiple providers.
EMRs check interactions only using the limited information within that clinic.
4. Care Planning and Documentation
EHR tools often include:
- Standardized nursing care plans
- Clinical decision support prompts
- Alerts for overdue interventions, vaccines, or screenings
These features streamline nursing documentation and improve quality metrics, reducing charting time and supporting safer patient care.
5. Patient Engagement
EHRs typically include patient portals where individuals can:
- View lab results
- Request medication refills
- Send messages to nurses or providers
This enhances communication and reduces administrative workload for nursing staff—a benefit not offered by most EMR systems.
ehr vs emr: Which should a nursing student learn for clinical rotations?
Nursing students entering clinical rotations often face the challenge of navigating multiple digital documentation platforms. Understanding the ehr vs emr distinction is crucial because it directly impacts how students document patient encounters, interpret clinical data, and coordinate care. While EMRs and EHRs both store patient information electronically, the scope, functionality, and interoperability differ, shaping the way nurses interact with patient records in practice.
An emr system is the digital representation of a patient’s chart within a single clinic or healthcare organization. It allows nursing students to perform essential tasks such as documenting vital signs, recording medication administration, updating patient progress notes, and reviewing prior lab results from that facility. For example, a student in a surgical unit might use the EMR to log post-operative assessments, track pain scores, and record wound evaluations. Mastery of these EMR functions ensures compliance with documentation standards, supports legal accountability, and allows students to participate safely in patient care.
However, many clinical rotations now take place in multi-facility networks or integrated health systems where ehr software is used. Unlike EMRs, EHRs aggregate patient information from multiple healthcare providers and organizations, providing a comprehensive view of a patient’s longitudinal medical history. Nursing students who learn to navigate EHR software can access laboratory results, imaging reports, medication histories, and specialist consults from other institutions—capabilities that an EMR alone may not provide.
Should I focus on learning emr system functions or ehr software features?
The focus for nursing students should be both practical and strategic. Competence in the emr system ensures students can accurately perform day-to-day documentation tasks, understand unit-specific workflows, and maintain legally sound records. For example, when charting vital signs or entering medication administration, the EMR provides structured fields that must be used correctly to maintain patient safety and ensure the accuracy of clinical data.
Simultaneously, familiarity with ehr software equips students to handle complex care coordination tasks. EHRs allow nurses to reconcile medications from multiple providers, verify external lab results, and follow chronic disease management plans across care settings. For instance, a nursing student on a cardiology rotation may need to view outpatient cardiology consults, previous echocardiograms from another hospital, and lab results from an independent laboratory. By understanding how to navigate EHR software, students can integrate all this information into clinical decision-making, improving workflow efficiency and patient safety.
How does understanding the difference between ehr and emr improve patient care?
Learning to understand the difference between EMRs and EHRs is more than a technical exercise; it directly impacts better patient care. EMRs provide essential documentation within a single organization, but they are limited in scope. EHRs, by contrast, consolidate information across providers and settings, enabling more informed clinical decisions. Nursing students who recognize these distinctions can identify gaps in patient information, reconcile conflicting data, and support continuity of care.
Example in practice: Consider a patient taking multiple medications prescribed by different specialists. If a nursing student relies solely on the local EMR, they may miss a medication prescribed elsewhere, increasing the risk of adverse interactions. Using EHR software, however, allows access to a complete medication list from several providers, ensuring safe administration and accurate patient education. Similarly, students can review outside lab results, past hospitalizations, and specialist notes before implementing nursing interventions, providing a holistic picture of the patient’s overall health.
Understanding ehr vs emr also enhances interdisciplinary collaboration. Nurses frequently communicate with physicians, pharmacists, and therapists; knowing which system contains the most complete information ensures accurate handoffs, reduces duplication of tests, and supports timely interventions. For nursing students, integrating this knowledge into clinical rotations promotes critical thinking, strengthens patient safety, and contributes to measurable improvements in outcomes.
How do electronic records impact patient data sharing and interoperability?
The adoption of electronic records has dramatically transformed the way healthcare systems store, access, and share patient information. For nursing students, understanding the implications of electronic documentation is critical, as accurate and timely data access directly influences clinical decision-making, patient safety, and workflow efficiency. Electronic records provide structured storage of clinical data, including vital signs, diagnoses, medications, and diagnostic results, enabling nurses and other care team members to quickly retrieve comprehensive patient information without sifting through paper charts. This digitization reduces errors, supports continuity of care, and enhances accountability within healthcare settings.
Beyond documentation, electronic records facilitate the interchangeably use of data across care teams and between institutions. Unlike traditional paper charts, which are static and often fragmented, electronic systems enable real-time access, updates, and secure communication of patient information. This interoperability is particularly relevant when patients receive care from multiple healthcare providers and organizations, such as specialists, hospitals, outpatient clinics, and laboratories.
How do ehrs enable interchangeably sharing of health information across health systems?
A key advantage of EHRs is their ability to consolidate and share health information across multiple platforms, ensuring that every provider involved in a patient’s care has access to the most accurate, up-to-date data. EHR data can include longitudinal records, medication histories, lab results, imaging, allergies, and prior diagnoses, creating a holistic view of the patient’s overall health.
Example: Consider a patient with diabetes who receives care at a primary care clinic, a cardiology specialty clinic, and a hospital. An EHR allows a nursing student to access the patient’s glucose logs, recent HbA1c results, cardiology consults, and hospital discharge summaries—all in one place. This capability not only improves clinical decision-making but also supports care coordination by ensuring that every healthcare professional has consistent information, reducing duplicative testing and medication errors.
What are the limits of emrs for medical information exchange between clinics?
While EMRs offer robust documentation within a single organization, their scope is limited. EMRs typically store data only within the clinic or hospital where it was created. As a result, transferring patient information between clinics, hospitals, or specialty centers often requires manual processes such as secure email, fax, or physical transfer of printed documents.
Example: A patient admitted to a hospital from an urgent care clinic may have vital lab results, imaging, or allergy information that is unavailable in the hospital EMR. Nurses must then actively seek these records from external sources, increasing the risk of incomplete information or delays in treatment. Understanding these limitations allows nursing students to recognize potential gaps in patient records and proactively verify critical information to maintain patient safety.
How does ehr data support care coordination and clinician communication?
EHRs enhance care coordination by creating a shared, longitudinal record accessible to all members of the healthcare team. Nursing students can leverage ehr data to review prior diagnoses, medications, lab results, and treatment plans, ensuring that interventions are accurate and consistent across care settings.
Example: In a postoperative scenario, a nurse can access EHR data to verify the patient’s preoperative labs, allergies, surgical history, and anesthesia records. Simultaneously, the surgeon, anesthesiologist, and physical therapist can input updates on progress, pain management, and mobility restrictions. This integrated approach improves communication between providers, reduces errors, and facilitates timely adjustments to the care plan.
Additionally, EHRs allow healthcare providers and organizations to track outcomes, monitor adherence to care protocols, and generate reports that inform quality improvement initiatives. For nursing students, familiarity with these tools is essential for effective patient care, as it allows them to anticipate gaps, validate information, and support clinical decision-making with accurate, comprehensive data.
What are practical tips for nursing students using ehr and emr systems?
Navigating emr and electronic health record systems can initially be challenging for nursing students, especially during clinical rotations in diverse healthcare settings. Developing proficiency with these systems is essential for safe patient care, accurate documentation, and effective communication with the interdisciplinary team. The following practical tips provide guidance on documenting, navigating, and maintaining privacy in digital health environments.
How to document accurate health history and patient’s health details in digital records?
Accurate documentation of a patient’s health history is the foundation of quality nursing care. Nursing students should focus on:
- Collecting comprehensive information: Include past diagnoses, medications, allergies, surgical history, and social determinants of health. For instance, when admitting a patient with diabetes, record prior HbA1c levels, insulin regimens, and recent hospitalizations to ensure continuity of care.
- Using structured templates: Most EHRs provide standardized forms and flow sheets. Using these templates ensures that critical elements like vitals, medication reconciliation, and clinical notes are consistently documented.
- Maintaining clarity and objectivity: Document observations factually rather than subjectively. Example: Instead of writing “patient seems anxious,” use “patient reports feeling anxious and has a heart rate of 102 bpm.”
- Regular updates: Record changes in the patient’s status in real time to maintain an up-to-date digital record. Delayed documentation can lead to errors in clinical decision-making.
How to navigate common ehr software tasks used by healthcare professionals?
Familiarity with electronic health record software functions improves efficiency and confidence during clinical rotations. Key tasks include:
- Patient lookup and record access: Learn to search by patient ID, name, or date of birth to quickly locate relevant records.
- Chart review: Review previous encounters, lab results, imaging studies, and medication history before initiating care. This helps prevent redundant testing and ensures informed clinical decisions.
- Order entry and documentation: Understand how to enter vital signs, assessments, and nursing notes accurately. For example, entering accurate intake/output data helps the care team monitor fluid balance in a patient with renal issues.
- Task management and alerts: EHRs often include reminders for overdue labs, medication administration, or patient education. Nursing students should learn to interpret and act on these alerts to support healthcare professionals in patient management.
- Interdisciplinary communication: Use messaging features within EHR software to communicate effectively with physicians, pharmacists, and other team members.
What privacy and security practices should a care provider follow with electronic health records?
Protecting patient information is a fundamental responsibility for all care providers. Nursing students must understand privacy requirements when using digital records:
- Access control: Only access records of patients under your care. Avoid “browsing” unrelated charts.
- Secure login: Use unique usernames and strong passwords; log out or lock the system when away from the workstation.
- HIPAA and institutional policies: Follow federal regulations and hospital policies regarding patient confidentiality. Never share login credentials or leave patient information visible on screens.
- Proper documentation practices: Avoid including unnecessary identifiers in notes or screenshots when sharing cases for learning purposes.
- Audit awareness: Many EHRs track user activity. Understand that your entries are monitored, emphasizing the importance of accuracy, professionalism, and confidentiality.
Example: A student documenting a post-operative patient should ensure that vital signs, wound assessments, and medication administration are recorded in the EHR immediately and accurately. Unauthorized access to another patient’s record, even inadvertently, can lead to serious legal and ethical consequences.
Conclusion
Navigating emr and electronic health record systems is a critical competency for nursing students, shaping how patient care is documented, communicated, and coordinated across healthcare settings. Understanding the distinctions between EMRs and EHRs—the ehr vs emr debate—is essential not only for accurate documentation but also for ensuring continuity of care, enhancing patient safety, and supporting interdisciplinary collaboration.
Through careful and accurate recording of a patient’s health history, effective use of digital records, and adherence to privacy and security protocols, nursing students can contribute meaningfully to clinical workflows while maintaining professionalism and compliance with healthcare regulations. Mastering common ehr software tasks, including reviewing labs, documenting interventions, and leveraging decision-support tools, empowers students to participate confidently in patient care and supports the work of healthcare professionals across multiple care settings.
Practical familiarity with EMRs in single organizations, coupled with proficiency in EHRs that enable interchangeably sharing health information across healthcare providers and organizations, ensures that nursing students are prepared for real-world clinical environments. By integrating these skills, students not only improve their own efficiency but also directly contribute to better patient care through enhanced communication, reduced errors, and coordinated interventions.
Ultimately, competence in EMR and EHR systems represents more than technical skill—it reflects a commitment to patient-centered care, evidence-based practice, and professional excellence. For nursing students, developing these capabilities early in their training lays the foundation for a career in which technology and clinical expertise intersect to optimize patient outcomes and strengthen the overall quality of healthcare delivery.
Frequently Asked Questions
What is the difference between EHR and EMR with example?
An EMR (Electronic Medical Record) is a digital version of a patient’s chart used within a single healthcare organization, primarily for documentation and clinical data tracking. An EHR (Electronic Health Record) goes beyond one practice and is designed to be shared across multiple healthcare providers and organizations, enabling coordinated care.
Example: A primary care clinic uses an EMR to record a patient’s blood pressure and medications. If the patient visits a cardiologist at another hospital, an EHR allows the cardiologist to access the patient’s complete history from both locations.
Is Epic an EHR or EMR?
Epic is an EHR system because it supports multi-facility data sharing, longitudinal patient records, and interoperability across different healthcare providers and organizations.
What does EHR stand for?
EHR stands for Electronic Health Record.
What is another name for EMR?
Another name for EMR is Electronic Medical Record, sometimes referred to simply as a digital chart within a single healthcare practice.