Nursing Care Plan for Multiple Sclerosis: Causes, Symptoms, & Interventions
Disclaimer: The information presented in this article is not medical advice; it is meant to act as a study guide for nursing students only. Please consult a registered physician for medical advice.
Introduction to Multiple Sclerosis (MS)
Multiple sclerosis (MS) is a chronic, progressive autoimmune disease that affects the central nervous system (brain, spinal cord, and optic nerves). It disrupts the flow of information within the brain, and between the brain and body.
Pathophysiology: MS occurs when the immune system mistakenly attacks myelin, the fatty substance that wraps around nerve fibers to protect them. This process is called demyelination. Without this outer shell, the nerves become damaged, and scar tissue (sclerosis) forms. This damage disrupts the electrical signals required for the body to move and feeClinical Manifestations (Symptoms)
The effects of MS vary widely among individuals. Symptoms often manifest between ages 20 and 40 and may include:
- Motor: Muscle weakness, spasms, tremors, and difficulty walking (ataxia).
- Sensory: Numbness, tingling (paresthesia), and pain.
- Visual: Blurred vision, double vision (diplopia), or optic neuritis.
- Cognitive: “Brain fog,” depression, and memory issues.
- Autonomic: Bladder/bowel dysfunction and sexual dysfunction.
Causes and Risk Factors
While the exact etiology is unknown, MS is likely caused by a combination of genetic and environmental factors:
- Viral Infections: Exposure to Epstein-Barr virus (EBV) or human herpesvirus 6 may trigger the immune system.
- Vitamin D Deficiency: Lower levels of Vitamin D and lack of sunlight exposure are correlated with higher MS rates.
- Genetics: Family history increases susceptibility.
- Smoking: Smoking may raise the risk and accelerate disease progression.
Diagnostic Evaluation
Diagnosis is challenging as symptoms mimic other neurological disorders. A neurologist will typically use the McDonald Criteria, which requires evidence of damage in at least two separate areas of the CNS at two different times.
Common Diagnostic Tests:
- MRI (Magnetic Resonance Imaging): The gold standard for detecting lesions (plaques) in the CNS.
- Lumbar Puncture (Spinal Tap): Analysis of cerebrospinal fluid (CSF) to detect oligoclonal bands (specific proteins found in MS).
- Evoked Potential Tests: Measures the speed of electrical signals in the brain.
Medical Management & Pharmacology
There is no cure, but treatment focuses on speeding recovery from attacks, slowing the progression of the disease, and managing symptoms.
Disease-Modifying Therapies (DMTs)
These drugs prevent relapses and slow disability progression:
- Injectables: Beta interferons (Avonex, Rebif), Glatiramer acetate (Copaxone).
- Oral: Dimethyl fumarate (Tecfidera), Teriflunomide (Aubagio).
- Infusions: Ocrelizumab (Ocrevus), Natalizumab (Tysabri).
Symptom Management
- Corticosteroids: Methylprednisolone (Solu-Medrol) for acute exacerbations (relapses).
- Muscle Relaxants: Baclofen or Tizanidine for spasticity.
- Stimulants: Modafinil for fatigue.
Nursing Care Plan for Multiple Sclerosis
Below are the prioritized nursing diagnoses and interventions for MS patients.
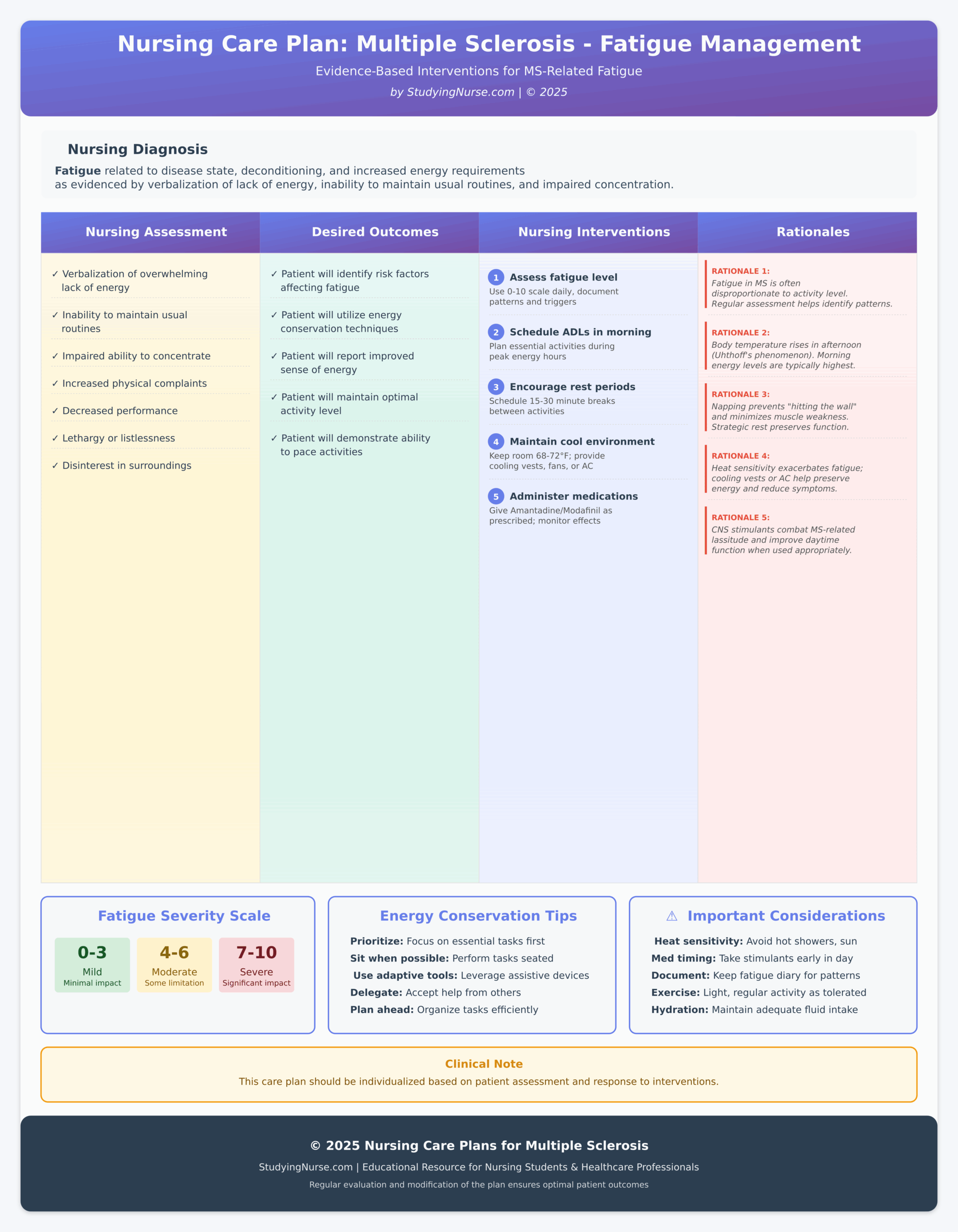
1. Nursing Care Plan: Fatigue
Nursing Diagnosis: Fatigue r/t disease state, deconditioning, and increased energy requirements.
| Nursing Assessment | Desired Outcomes | Nursing Interventions | Rationales |
| • Verbalization of overwhelming lack of energy. • Inability to maintain usual routines. • Impaired ability to concentrate. • Increased physical complaints. | • Patient will identify risk factors affecting fatigue. • Patient will utilize energy conservation techniques. • Patient will report an improved sense of energy. | 1. Assess fatigue level (0-10 scale). | Fatigue in MS is often disproportionate to activity level and is not always related to physical disability. |
| 2. Schedule ADLs in the morning. | Body temperature often rises in the afternoon, which can worsen fatigue (Uhthoff’s phenomenon). | ||
| 3. Encourage rest periods. | Napping or resting prevents “hitting the wall” and minimizes the aggravation of muscle weakness. | ||
| 4. Maintain cool environment. | Heat sensitivity exacerbates MS fatigue; cooling vests or air conditioning can help preserve energy. | ||
| 5. Administer meds (Amantadine/Modafinil). | CNS stimulants can help combat MS-related lassitude and improve daytime function. |
🏥 Nursing Care Plan: Multiple Sclerosis – Fatigue Management
📋 Nursing Diagnosis
| 🔍 Nursing Assessment | 🎯 Desired Outcomes | 💊 Nursing Interventions | 📚 Rationales |
|---|---|---|---|
|
|
1
Assess fatigue level (0-10 scale)
Evaluate fatigue severity at same time daily, document patterns and triggers
2
Schedule ADLs in the morning
Plan essential activities during peak energy hours (typically morning)
3
Encourage rest periods
Schedule 15-30 minute rest breaks between activities; promote short naps if needed
4
Maintain cool environment
Keep room temperature 68-72°F; provide cooling vests, fans, or AC as needed
5
Administer medications
Give Amantadine or Modafinil as prescribed; monitor effectiveness and side effects
|
Rationale 1:
Fatigue in MS is often disproportionate to activity level and is not always related to physical disability. Regular assessment helps identify patterns.
Rationale 2:
Body temperature often rises in the afternoon, which can worsen fatigue (Uhthoff’s phenomenon). Morning energy levels are typically highest.
Rationale 3:
Napping or resting prevents “hitting the wall” and minimizes the aggravation of muscle weakness. Strategic rest preserves function.
Rationale 4:
Heat sensitivity exacerbates MS fatigue; cooling vests or air conditioning can help preserve energy and reduce symptom severity.
Rationale 5:
CNS stimulants can help combat MS-related lassitude and improve daytime function when used appropriately.
|
📊 Fatigue Severity Scale
Use this scale to assess and document fatigue levels:
💡 Energy Conservation Tips
- Prioritize: Focus on essential tasks first
- Sit when possible: Perform tasks while seated
- Use adaptive tools: Leverage assistive devices
- Delegate: Accept help from others
⚠️ Important Considerations
- Heat sensitivity: Avoid hot showers, direct sun
- Medication timing: Take stimulants early in day
- Document: Keep fatigue diary for patterns
- Exercise: Light, regular activity as tolerated
2. Nursing Care Plan: Self-Care Deficit
Nursing Diagnosis: Self-care deficit (feeding, bathing, dressing) r/t neuromuscular impairment and spasticity.
| Nursing Assessment | Desired Outcomes | Nursing Interventions | Rationales |
| • Inability to perform ADLs. • Frustration or depression. • Poor personal hygiene. • Tremors or weakness. | • Patient will perform self-care within level of ability. • Patient will identify resources for assistance. • Patient will remain free of skin breakdown. | 1. Promote autonomy. | Encourage the patient to do as much as possible to maintain muscle tone and self-esteem. Do not rush them. |
| 2. Provide assistive devices. | Weighted utensils, shower chairs, and zipper pulls can compensate for tremors and weakness. | ||
| 3. Administer Antispasmodics (Baclofen). | Reducing spasticity facilitates smoother movement, making dressing and bathing easier. | ||
| 4. Implement skincare routine. | Immobility increases pressure ulcer risk; frequent repositioning protects the sacrum and heels. |
😓 Struggling with this Care Plan?
Save time and stress. Get a custom, plagiarism-free nursing paper written by our BSN & MSN experts.
✍️ Write My Care Plan100% Confidential • 20% OFF Code: NURSE20
3. Nursing Care Plan: Risk for Caregiver Role Strain
Nursing Diagnosis: Risk for Caregiver Role Strain r/t complexity of care and progressive disability.
| Nursing Assessment | Desired Outcomes | Nursing Interventions | Rationales |
| • Caregiver expresses burnout or stress. • Duration of care required. • Lack of respite services. | • Caregiver will identify resources for support. • Caregiver will report satisfaction with the care plan. • Caregiver will engage in self-care. | 1. Assess caregiver burden. | Identifying the level of stress early prevents burnout and potential neglect. |
| 2. Facilitate respite care. | Caregivers need time away to recharge; identify day-care centers or other family members to assist. | ||
| 3. Teach safe transfer techniques. | Proper body mechanics prevent injury to both the patient and the caregiver. | ||
| 4. Refer to support groups. | Connecting with others in similar situations reduces isolation and provides emotional outlet. |
4. Nursing Care Plan: Impaired Urinary Elimination
Nursing Diagnosis: Impaired Urinary Elimination r/t neurogenic bladder dysfunction.
| Nursing Assessment | Desired Outcomes | Nursing Interventions | Rationales |
| • Incontinence or retention. • Nocturia (nighttime voiding). • Recurrent UTIs. • Bladder distention. | • Patient will empty bladder completely. • Patient will remain free of UTIs. • Patient will demonstrate self-catheterization if needed. | 1. Palpate bladder after voiding. | Checks for retention/residual urine which increases infection risk. |
| 2. Implement timed voiding. | Creates a schedule to train the bladder and reduce incontinence episodes. | ||
| 3. Push fluids (2-3L/day). | Dilutes urine and flushes bacteria; avoid caffeine/alcohol as they act as diuretics/irritants. | ||
| 4. Teach intermittent catheterization. | May be required for flaccid bladder (retention) to ensure complete emptying. | ||
| 5. Administer Anticholinergics (Oxybutynin). | Relaxes bladder muscles to treat spastic bladder (urgency/frequency). |
5. Nursing Care Plan: Powerlessness
Nursing Diagnosis: Powerlessness r/t progressive, unpredictable nature of the disease.
| Nursing Assessment | Desired Outcomes | Nursing Interventions | Rationales |
| • Verbal expression of lack of control. • Depression or passivity. • Nonparticipation in care decisions. | • Patient will identify areas of control. • Patient will participate in decision-making. • Patient will verbalize feelings. | 1. Acknowledge feelings. | Validating the patient’s fear helps build trust and reduces anxiety. |
| 2. Involve patient in planning. | Giving the patient choices (e.g., time of bath) restores a sense of control. | ||
| 3. Focus on current abilities. | Emphasize what the patient can still do rather than what they have lost. | ||
| 4. Refer to counseling. | Professional support helps process the grief associated with chronic illness. |
Frequently Asked Questions (FAQ)
What are the first signs of Multiple Sclerosis?
The early signs often include vision problems (optic neuritis), numbness or tingling in the limbs, unexplained fatigue, and balance issues. These symptoms may appear and disappear (relapsing-remitting).
What is the main cause of MS?
The exact cause is unknown (idiopathic), but it is considered an autoimmune reaction where the body attacks its own myelin. It is triggered by a combination of genetics, viral infections (like EBV), and environmental factors (low Vitamin D).
What is the life expectancy for someone with MS?
With modern treatments, the life expectancy for MS patients is near normal—typically about 7 years less than the general population. Death usually results from complications like infection or immobility rather than the disease itself.
Can MS be cured?
Currently, there is no cure for MS. However, Disease-Modifying Therapies (DMTs) are highly effective at slowing the progression of the disease and reducing the frequency of relapses.
Read More Nursing Care Plans: