A Diabetes SOAP Note is a structured method of documentation used by healthcare providers to record patient information, observations, and treatment plans specifically for patients with diabetes mellitus type 2. This standardized format ensures that all essential aspects of a patient’s diabetic condition are consistently captured and communicated among healthcare professionals.
SOAP stands for Subjective, Objective, Assessment, and Plan. In the context of diabetes management, a SOAP note helps healthcare providers track the progress of a patient’s condition, monitor treatment effectiveness, and make informed decisions about ongoing care.
Components of a SOAP Note
- Subjective: This section includes the patient’s reported symptoms, concerns, and experiences related to their diabetes. It may cover aspects such as fatigue, increased thirst (polydipsia), frequent urination (polyuria), blurred vision, or any other symptoms associated with diabetes type 2.
- Objective: This component documents measurable and observable data, including vital signs, physical examination findings, and laboratory results. For diabetes patients, this often includes blood glucose levels, hemoglobin A1C results, blood pressure readings, and weight.
- Assessment: In this section, the healthcare provider evaluates the patient’s condition based on the subjective and objective information gathered. It may include the current status of diabetes management, potential complications, and any new or ongoing issues related to the patient’s diabetes.
- Plan: The final section outlines the treatment plan, including any adjustments to medications, lifestyle modifications, follow-up appointments, and patient education needs.
Diabetes SOAP Note Example
SUBJECTIVE:
Chief Complaint: “My blood sugar has been really high for the past week, and I feel very thirsty”
History of Present Illness:
58-year-old male with Type 2 Diabetes Mellitus (diagnosed 5 years ago) presents with one week of elevated blood glucose readings (ranging 250-400 mg/dL), increased thirst, frequent urination, and fatigue. Patient reports poor medication adherence over the past month due to financial constraints. Denies fever, chest pain, or shortness of breath. Has been drinking more water but hasn’t modified diet. Denies recent illness or new medications.
Current Medications:
- Metformin 1000mg BID (reports missing ~50% of doses in past month)
- Glipizide 10mg daily (reports missing ~50% of doses in past month)
- Lisinopril 10mg daily for hypertension
Allergies: NKDA
Review of Systems:
Positive:
- Constitutional: Fatigue, polydipsia
- Urinary: Polyuria
- Endocrine: Polyphagia
Negative: - No chest pain, shortness of breath, nausea, vomiting
- No visual changes
- No numbness/tingling in extremities
- No wounds or infections
OBJECTIVE:
Vital Signs:
- BP: 142/88 mmHg
- HR: 88 bpm
- RR: 16/min
- Temp: 98.6°F
- SpO2: 98% on room air
- Weight: 92 kg (stable)
Physical Examination:
General: Alert, oriented, no acute distress
HEENT: Mucous membranes slightly dry
Cardiovascular: Regular rate and rhythm, no murmurs
Respiratory: Clear to auscultation bilaterally
Abdominal: Soft, non-tender, non-distended
Skin: No lesions or infections
Neurological: Alert, oriented x3, intact sensation
Extremities: No edema, no ulcers
Laboratory Results:
- Point of care glucose: 342 mg/dL
- HbA1c: 10.2% (previous was 7.8% three months ago)
- Basic Metabolic Panel:
- Sodium: 138 mEq/L
- Potassium: 4.2 mEq/L
- Chloride: 102 mEq/L
- CO2: 24 mEq/L
- BUN: 18 mg/dL
- Creatinine: 1.1 mg/dL
- Calculated osmolality: 295 mOsm/kg
- Urinalysis: Glucose 3+, no ketones
- Urine microalbumin: 45 mg/24h
ASSESSMENT:
Primary Diagnosis:
- Type 2 Diabetes Mellitus with Hyperglycemia (E11.65)
Rationale: Elevated blood glucose, increased HbA1c, symptoms of hyperglycemia, and known history of T2DM
Contributing Factors:
- Medication non-adherence due to financial constraints
- Poor dietary control
- Possible medication resistance
Differential Diagnoses:
- Diabetic Ketoacidosis (E11.10)
Rationale: Ruled out by absence of ketones, normal pH, and mental status - Hyperosmolar Hyperglycemic State (E11.00)
Rationale: Ruled out by normal osmolality and mental status - New-onset infection (R50.9)
Rationale: Ruled out by normal temperature and absence of symptoms
Complications Assessment:
- Early diabetic nephropathy (elevated urine microalbumin)
- No current diabetic retinopathy or neuropathy
PLAN:
Medications:
- Resume previous doses of Metformin and Glipizide
- Add Empagliflozin 10mg daily (provided samples for 1 month)
- Continue Lisinopril 10mg daily
Rationale: Add SGLT2 inhibitor to improve glycemic control
Laboratory Monitoring:
- Basic metabolic panel in 1 week
- HbA1c repeat in 3 months
- Comprehensive metabolic panel in 1 month
Rationale: Monitor response to therapy and assess organ function
Diabetes Management:
- Provided glucometer and testing supplies
- Instructions for blood glucose monitoring 4x daily
- Target blood glucose: 80-130 mg/dL fasting, <180 mg/dL post-prandial
Rationale: Enable proper self-monitoring
Education:
- Detailed dietary counseling with emphasis on carbohydrate counting
- Referral to diabetes educator
- Signs/symptoms of hyper/hypoglycemia reviewed
Rationale: Improve self-management skills
Social Support:
- Referral to social worker for medication assistance programs
- Provided information about generic medication options
Rationale: Address financial barriers to care
Follow-up:
- Return visit in 1 week
- Call office if blood glucose >400 mg/dL or symptoms worsen
- Provided after-hours contact information
Patient Understanding:
Patient verbalizes understanding of medication changes, glucose monitoring, and follow-up plan. Agrees to contact office if symptoms worsen.
Time Spent: 30 minutes
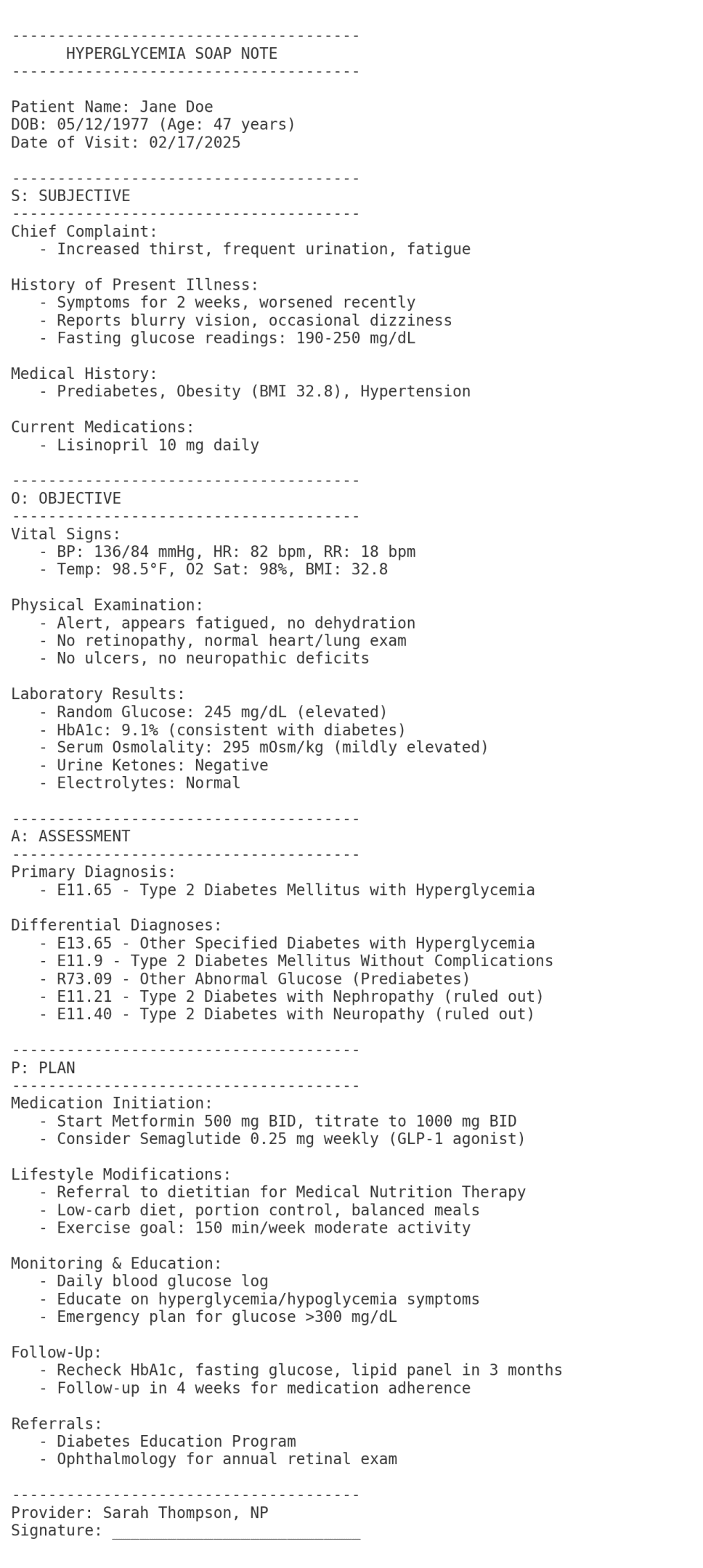
Hyperglycemia SOAP Note Example
S: Subjective
Chief Complaint: “I’ve been extremely thirsty, urinating a lot, and feeling tired for the past week.”
HPI:
- 48-year-old female with 7-day history of polyuria, polydipsia, fatigue, and blurred vision.
- Reports unintentional weight loss of 4 lbs over 2 weeks.
- Denies nausea, vomiting, abdominal pain, or recent illness.
- No history of diabetes. Family history: Mother with type 2 diabetes.
- Diet: High in sugary snacks and fast food; minimal physical activity.
PMH: Hypertension, obesity (BMI 32).
Medications: Lisinopril 10 mg daily.
Allergies: NKDA.
Social: Smokes ½ pack/day; denies alcohol/drug use.O: Objective
Vital Signs:
- Temp: 98.6°F (oral)
- HR: 88 bpm
- RR: 16/min
- BP: 142/88 mmHg
- Weight: 88 kg
- Blood Glucose (fingerstick): 298 mg/dL (fasting)
Physical Exam:
- General: Alert, obese, fatigued appearance.
- HEENT: Dry mucous membranes; no acanthosis nigricans.
- Cardiac: Regular rate/rhythm, no murmurs.
- Abdomen: Soft, non-tender, no hepatomegaly.
- Skin: No lesions or infections; poor skin turgor.
- Neurologic: Alert, oriented; no focal deficits.
Labs (if available):
- HbA1c: 9.2% (elevated, indicative of chronic hyperglycemia)
- Urinalysis: Glucose 3+, no ketones.
- Basic Metabolic Panel: Serum glucose 310 mg/dL, normal anion gap.
A: Assessment
Primary Diagnosis:
- Hyperglycemia, likely due to New-Onset Type 2 Diabetes Mellitus (ICD-10: R73.9 – Hyperglycemia, unspecified; E11.65 – Type 2 DM with hyperglycemia if confirmed)
- Rationale:
- Classic symptoms (polyuria, polydipsia, weight loss) + fasting glucose >126 mg/dL and HbA1c ≥6.5%.
- No ketones or metabolic acidosis to suggest DKA.
Differential Diagnoses:
- Diabetic Ketoacidosis (DKA) (ICD-10: E11.10)
- Rationale for Exclusion: Absent ketones, normal anion gap, no acidosis.
- Hyperosmolar Hyperglycemic State (HHS) (ICD-10: E11.00)
- Rationale for Exclusion: Serum osmolality not severely elevated; patient alert.
- Secondary Hyperglycemia (e.g., steroid use, infection) (ICD-10: R73.9)
- Rationale for Exclusion: No recent steroid use; urinalysis negative for infection.
P: Plan
- Immediate Interventions:
- Hydration: Encourage oral fluids (water); monitor for signs of dehydration.
- Blood Glucose Monitoring: Teach home glucose checks (fasting and 2 hours postprandial).
- Medications:
- Metformin 500 mg PO BID (start after confirming renal function is normal).
- Rationale: First-line for type 2 diabetes; improves insulin sensitivity.
- Lifestyle Modifications:
- Dietary Counseling: Refer to dietitian for low-carbohydrate, high-fiber meal planning.
- Exercise: Encourage 30 minutes of daily walking.
- Education:
- Teach signs of DKA/HHS (e.g., vomiting, confusion) and when to seek emergency care.
- Smoking cessation counseling (nicotine replacement therapy offered).
- Follow-Up:
- Repeat HbA1c in 3 months.
- PCP follow-up in 1 week for medication adherence and glucose logs.
- Ophthalmology referral for blurred vision (rule out diabetic retinopathy).
- Monitoring:
- Renal function tests (BUN/Cr) before starting metformin.
- Foot exam for neuropathy at next visit.
Rationale for ICD-10 Selection:
- R73.9: Initial code for hyperglycemia without confirmed diabetes.
- E11.65: Used if type 2 diabetes is confirmed (pending further evaluation).
- Differentials excluded based on labs, exam, and history.
Clinical Decision-Making:
- Hyperglycemia likely reflects undiagnosed type 2 diabetes given risk factors (obesity, family history). Immediate focus on glycemic control and lifestyle changes to prevent complications.
Mastering the diabetes SOAP note is an essential skill for nursing students entering clinical practice. A well-crafted diabetes SOAP note provides a comprehensive framework for documenting patient care, tracking progress, and ensuring proper diabetes management. As a nursing student, understanding how to properly document patient encounters related to diabetes mellitus can significantly impact patient outcomes and your professional development.
SOAP Note Structure
The SOAP note format has become the standard documentation method in healthcare settings. When applied to diabetes care, a diabetes SOAP note allows healthcare professionals to systematically record relevant information about patients with diabetes.

A SOAP note consists of four distinct components:
- S (Subjective): Information reported by the patient
- O (Objective): Measurable and observable data gathered during assessment
- A (Assessment): Clinical conclusions based on subjective and objective information
- P (Plan): Treatment strategies and next steps
For diabetes care, each component of the SOAP note addresses specific aspects of the condition, from symptoms to treatment plans. Let’s explore how to effectively document each section for patients with diabetes.
The Subjective Component of Diabetes SOAP Notes
The subjective section of a diabetes SOAP note captures the patient’s personal experience with their condition. This includes their chief complaints, symptoms, and how diabetes affects their daily life.
When documenting the subjective component for patients with diabetes, focus on:
- Symptoms of hyperglycemia: Patients may report polyuria, increased thirst, blurred vision, or fatigue
- Blood glucose monitoring: Patient-reported blood glucose levels and testing frequency
- Medication adherence: Information about insulin administration or oral medications
- Dietary habits: Food intake patterns and relationship to blood sugar levels
- Physical activity: Exercise routines and their effect on glucose control
- Recent changes: Any recent modifications to medication, diet, or lifestyle
{kind=link}
A thorough subjective section might include statements such as: “Patient reports blood glucose readings ranging from 180-250 mg/dL over the past week. Denies fever, chest pain, or shortness of breath. Patient admits to dietary non-compliance during weekend family gathering. Denies dizziness or abdominal pain.”
The Objective Component in Diabetes SOAP Notes
The objective section of a diabetes SOAP note documents clinical findings and measurable data. This critical component provides concrete evidence of the patient’s current health status.
Key elements to include in the objective section for diabetes care:
- Vital signs: Blood pressure (goal blood pressure for patients with diabetes is typically <140/90 mmHg), heart rate, respiratory rate, temperature
- Weight and BMI: Important for tracking changes over time
- Physical examination findings: Skin integrity, foot assessment, cardiovascular exam
- Laboratory results: HbA1c (target is generally less than 7%), fasting plasma glucose, oral glucose tolerance test results if applicable
- Blood glucose readings: Current readings and patterns from patient logs
- Medication review: Current diabetes medications including insulin types and dosages
For example: “Vital signs: BP 138/84 mmHg, HR 78, RR 16, Temp 98.6°F. Weight 192 lbs (no change from last visit). Random blood glucose: 187 mg/dL. HbA1c: 7.8% (increased from 7.2% three months ago). Physical exam reveals no acute findings. No signs of peripheral neuropathy. Foot exam shows intact skin, normal sensation.”
Assessment in Diabetes SOAP Notes
The assessment section synthesizes the subjective and objective information to form clinical judgments about the patient’s diabetes management. This section identifies problems and evaluates the patient’s condition in the context of diabetes.
Important considerations for the assessment section:
- Diabetes classification: Type 1 diabetes, type 2 diabetes, or gestational diabetes
- Glycemic control: Whether blood glucose levels are well-managed
- Complications: Presence of acute or chronic diabetes-related issues
- Risk factors: Identification of factors affecting diabetes management
- Comorbidities: Other conditions like hypertension or rheumatoid arthritis that may impact diabetes care
A comprehensive assessment might read: “58-year-old male with type 2 diabetes mellitus with suboptimal glycemic control evidenced by elevated blood glucose readings and increased HbA1c. Patient demonstrates adequate medication adherence but struggles with dietary compliance. No signs of acute complications. Hypertension is currently well-controlled.”
The Plan Component of Diabetes SOAP Notes
The plan section outlines the treatment strategy for managing the patient’s diabetes and related conditions. This section should be clear, specific, and actionable.
Elements to address in the plan section:
- Medication adjustments: Changes to insulin doses or oral agents
- Glucose monitoring: Recommendations for timing and frequency
- Lifestyle modifications: Dietary guidance, physical activity recommendations
- Education: Topics for diabetes self-management education
- Referrals: Consultations with specialists if needed
- Follow-up: Timing for next appointment and monitoring parameters
An effective plan might include: “1. Continue Metformin 1000mg BID. 2. Increase Glipizide to twice daily dosing. 3. Monitor blood glucose levels before meals and at bedtime. 4. Referral to diabetes educator for dietary counseling, focusing on whole grains and portion control. 5. Encourage 30 minutes of physical activity 5 days per week. 6. Reduce sodium intake to 2 grams daily to manage hypertension. 7. Return for follow-up in 1 month with blood glucose log.”
Diabetes SOAP Note Example for Type 2 Diabetes
To illustrate the application of the SOAP format in the context of diabetes, here’s an example diabetes SOAP note for a patient with type 2 diabetes:
S: 50-year-old African American male with type 2 diabetes presents for a routine follow-up. Reports average morning blood glucose readings of 150-180 mg/dL. Denies hypoglycemic episodes. States he has been “mostly” taking medications as prescribed but occasionally misses evening dose. Denies chest pain, shortness of breath, or blurred vision. Reports maintaining a healthy diet during weekdays but admits to poor choices on weekends. Currently walking 15 minutes daily.
O: Vital signs: BP 142/88 mmHg, HR 76, RR 18, Temp 98.4°F. Weight 202 lbs (up 3 lbs from last visit). Random plasma glucose: 163 mg/dL. HbA1c: 7.9% (previous was 7.5%). Current medications were mentioned: Metformin 1000mg BID, Glipizide 5mg daily, Lisinopril 10mg daily. Physical exam reveals normal heart sounds, clear lungs. Foot exam shows no lesions or decreased sensation. No edema noted.
A: Type 2 diabetes mellitus with worsening glycemic control. Contributing factors include medication non-adherence and inconsistent dietary habits. Hypertension borderline controlled. Weight gain since last visit indicating need for therapy in order to lower cardiovascular risk. No evidence of diabetic neuropathy or other acute complications.
P:
- Adjust Glipizide, increased to twice daily
- Emphasize medication adherence, especially evening doses
- Recommend drinking more water and limiting caloric beverages
- Encourage increased physical activity to 30 minutes daily
- SMART goal: Patient will track blood glucose levels 2 times daily for next 2 weeks
- Avoid drinking alcohol as it has a negative interaction with current medications
- Follow up in 4 weeks with blood glucose log
- Lab work including lipid panel and kidney function in 2 weeks to reduce CVD risks by maintaining healthy cholesterol levels
Type 1 Diabetes SOAP Note Considerations
While many aspects of documentation are similar, a diabetes SOAP note for type 1 diabetes has some unique considerations. Type 1 diabetes management differs significantly from type 2 diabetes management, primarily due to the absolute insulin deficiency.
In a SOAP note for type 1 diabetes:
- Subjective: Focus on insulin administration, carbohydrate counting, and hypoglycemic episodes
- Objective: Include insulin-to-carbohydrate ratios and correction factors
- Assessment: Address insulin management and technology use (pumps, continuous glucose monitors)
- Plan: Often includes more detailed insulin adjustments and hypoglycemia prevention strategies
Best Practices for Effective Diabetes SOAP Notes
To improve your diabetes SOAP note documentation, consider these best practices:
- Use specific, measurable terms: Instead of “high glucose,” document actual readings (e.g., “blood glucose 275 mg/dL”).
- Maintain chronological order: Present information in a logical sequence.
- Avoid subjective judgments: Focus on facts rather than assumptions about patient behavior.
- Document patient understanding: Note the patient’s comprehension of their condition and management plan.
- Address barriers to care: Identify factors affecting the patient’s ability to manage their diabetes.
- Use appropriate terminology: Accurately describe diabetes-related concepts using proper medical terminology.
Diabetes SOAP Note Template for Student Practice
To help nursing students practice documentation, here’s a basic diabetes SOAP note template:
S:
- Chief complaint
- History of present illness
- Diabetes history (type, duration, previous control)
- Current symptoms
- Medication adherence
- Dietary patterns
- Physical activity
- Self-monitoring practices
- Family history related to diabetes
- Psychosocial factors affecting diabetes management
O:
- Vital signs
- Height, weight, BMI
- General appearance
- Physical examination findings
- Blood glucose reading (current)
- Laboratory results
- Medication list
- Diabetes supplies and equipment
A:
- Diabetes type and control status
- Acute or chronic complications
- Contributing factors to current status
- Risk assessment
- Comorbidities
- Barriers to management
P:
- Medications (continue, adjust, discontinue)
- Monitoring recommendations
- Dietary modifications
- Physical activity recommendations
- Education provided
- Referrals
- Goals (SMART format)
- Follow-up timing and focus
How to Structure a Diabetes SOAP Note
When structuring a SOAP note for a patient with type 2 diabetes, it’s important to include specific information relevant to diabetes management. Here’s a general structure:
Subjective:
- Chief complaint or reason for visit
- Patient’s reported symptoms (e.g., polyuria, polydipsia, fatigue)
- Patient’s compliance with medication and lifestyle recommendations
- Any changes in diet or physical activity
- Stress levels or other factors affecting blood sugar control
Objective:
- Vital signs (blood pressure, heart rate, temperature, respiratory rate)
- Weight and BMI
- Blood glucose readings (fasting and postprandial)
- Recent A1C results
- Physical examination findings (e.g., foot exam, skin integrity)
- Results of any recent lab tests (e.g., lipid panel, kidney function tests)
Assessment:
- Current status of diabetes control (well-controlled, poorly controlled)
- Presence of any diabetes-related complications
- Evaluation of risk factors (e.g., hypertension, hyperlipidemia)
- Any new or ongoing issues related to diabetes management
Plan:
- Adjustments to medication regimen (if necessary)
- Recommendations for lifestyle modifications
- Referrals to specialists (e.g., endocrinologist, nutritionist)
- Patient education needs
- Follow-up appointment schedule
- Goals for next visit
What Should Be Included Comprehensive Soap Note for Diabetes Type 2?

Essential Patient Information for Diabetes SOAP Notes
When documenting a Diabetes SOAP note for a patient with diabetes type 2, it’s crucial to include the following essential patient information:
- Patient Demographics: Name, age, gender, and date of visit
- Diabetes History: Date of diagnosis, type of diabetes, and current treatment regimen
- Comorbidities: Other medical conditions that may affect diabetes management
- Family History: Especially related to diabetes and cardiovascular diseases
- Social History: Occupation, living situation, and any social factors affecting diabetes management
Documenting Current Medications in Diabetes Management
Accurately recording current medications is vital for effective diabetes management. Include:
- Diabetes-specific medications (e.g., Metformin, insulin)
- Dosage and frequency of each medication
- Any recent changes in medication regimen
- Patient’s adherence to prescribed medications
- Over-the-counter medications and supplements
- Medications for comorbid conditions (e.g., hypertension, hyperlipidemia)
Physical Examination Findings Relevant to Diabetes
A comprehensive physical examination for a patient with diabetes type 2 should include:
- General appearance and level of alertness
- Vital signs (blood pressure, heart rate, respiratory rate, temperature)
- Height, weight, and BMI calculation
- Cardiovascular examination (heart sounds, peripheral pulses)
- Respiratory examination
- Abdominal examination (checking for hepatomegaly or tenderness)
- Neurological examination (sensory and motor function, especially in extremities)
- Foot examination (checking for ulcers, infections, or neuropathy)
- Skin examination (looking for acanthosis nigricans, insulin injection sites)
- Eye examination (if possible, or noting recent ophthalmology visits)
How to Assess Blood Sugar Levels in Diabetes Type 2?
Monitoring Blood Glucose: Tools and Techniques
Assessing blood sugar levels is a crucial aspect of diabetes management. Here are some common tools and techniques:
- Glucometers: These portable devices allow patients to check their blood glucose levels at home using a small blood sample.
- Continuous Glucose Monitoring (CGM) Systems: These devices provide real-time glucose readings throughout the day and night, offering a more comprehensive view of glucose patterns.
- Fasting Plasma Glucose Test: This test measures blood sugar levels after an 8-hour fast, typically performed in a laboratory setting.
- Oral Glucose Tolerance Test (OGTT): This test involves measuring blood glucose levels before and 2 hours after consuming a glucose-rich drink.
- Random Plasma Glucose Test: This test can be done at any time of the day, regardless of when the patient last ate.
Understanding A1C Levels and Their Importance
Hemoglobin A1C (HbA1c) is a crucial marker for long-term blood glucose control:
- What is A1C?: It’s a blood test that reflects average blood glucose levels over the past 2-3 months.
- Target A1C: For most adults with diabetes, the target A1C is less than 7%. However, this may vary based on individual factors.
- Frequency of Testing: A1C is typically measured every 3-6 months, depending on how well the patient’s diabetes is controlled.
- Interpretation:
- Below 5.7%: Normal
- 5.7% to 6.4%: Prediabetes
- 6.5% or above: Diabetes
- Importance: Regular A1C testing helps healthcare providers assess the effectiveness of the current treatment plan and make necessary adjustments.
Identifying Symptoms of Hyperglycemia and Hypoglycemia
Recognizing the symptoms of high and low blood sugar is essential for both patients and healthcare providers:
Hyperglycemia (High Blood Sugar):
- Increased thirst (polydipsia)
- Frequent urination (polyuria)
- Fatigue
- Blurred vision
- Slow-healing wounds
- Recurrent infections
Hypoglycemia (Low Blood Sugar):
- Shakiness
- Sweating
- Rapid heartbeat
- Confusion
- Irritability
- Hunger
- Weakness
- In severe cases, loss of consciousness
What Lifestyle Modifications are Recommended for Patients with Diabetes?
Dietary Changes to Manage Diabetes Type 2
- Carbohydrate Management: Encourage patients to monitor their carbohydrate intake and choose complex carbohydrates over simple sugars.
- Portion Control: Teach patients about appropriate portion sizes to help manage calorie intake and blood sugar levels.
- Increased Fiber Intake: Recommend a diet rich in fiber, including whole grains, legumes, fruits, and vegetables.
- Limit Saturated and Trans Fats: Advise patients to reduce intake of saturated fats and eliminate trans fats to support heart health.
- Consistent Meal Timing: Encourage regular meal times to help maintain stable blood glucose levels.
- Hydration: Stress the importance of adequate water intake.
Importance of Physical Activity in Diabetes Management
Regular physical activity is crucial for managing diabetes type 2:
- Blood Glucose Control: Exercise helps lower blood glucose levels and improves insulin sensitivity.
- Weight Management: Physical activity aids in maintaining a healthy weight or achieving weight loss goals.
- Cardiovascular Health: Regular exercise reduces the risk of heart disease and stroke, common complications in diabetes.
- Stress Reduction: Physical activity can help manage stress, which can affect blood glucose levels.
- Recommendations: Aim for at least 150 minutes of moderate-intensity aerobic activity per week, spread over at least 3 days, with no more than 2 consecutive days without exercise.
Managing Hypertension and Cholesterol Levels
Controlling blood pressure and cholesterol is essential in diabetes management:
- Blood Pressure Goals: The target blood pressure for most patients with diabetes is below 140/90 mmHg.
- Cholesterol Management:
- LDL Cholesterol: Target is generally <100 mg/dL
- HDL Cholesterol: Target is >40 mg/dL for men and >50 mg/dL for women
- Triglycerides: Target is <150 mg/dL
- Lifestyle Modifications:
- Reduce sodium intake
- Increase consumption of fruits, vegetables, and whole grains
- Limit alcohol consumption
- Quit smoking
- Medication: If lifestyle changes are insufficient, medications may be prescribed to manage hypertension and hyperlipidemia.
How to Document a Patient’s History of Present Illness?
Key Questions to Ask During Patient Assessment
When documenting the history of present illness for a patient with diabetes type 2, consider asking the following key questions:
- What brings you in today? Are you experiencing any new symptoms?
- How well controlled do you feel your blood sugar has been recently?
- Have you had any episodes of very high or very low blood sugar?
- Are you experiencing any symptoms like increased thirst, frequent urination, or blurred vision?
- Have you noticed any changes in your energy levels or weight?
- Are you having any problems with your feet, such as numbness, tingling, or wounds that won’t heal?
- Have you been able to follow your diet and exercise plan?
- Are you taking your medications as prescribed? Any side effects?
- Have you had any recent illnesses or stressors that might have affected your blood sugar?
- When was your last eye exam?
Identifying Common Complaints in Type 2 Diabetes Patients
Common complaints that should be noted in the history of present illness include:
- Fatigue or lack of energy
- Increased thirst and frequent urination
- Blurred vision
- Slow-healing wounds
- Numbness or tingling in hands or feet
- Recurrent infections (e.g., urinary tract infections, skin infections)
- Unexplained weight loss or gain
- Difficulty managing blood sugar levels
- Side effects from diabetes medications
- Stress or anxiety related to diabetes management
Recording Patient Reports: What to Include
When documenting patient reports in the SOAP note, include:
- The patient’s description of their symptoms in their own words
- The duration and frequency of reported symptoms
- Any factors that worsen or alleviate the symptoms
- The impact of symptoms on daily activities and quality of life
- Any self-management strategies the patient has tried
- The patient’s perception of their diabetes control
- Any concerns or questions the patient has about their condition
- Recent changes in lifestyle, diet, or medication adherence
- Any recent stressors or life events that may be affecting diabetes management
- The patient’s goals for their diabetes care
What are the Common Complications in Diabetes Type 2?
Recognizing Diabetic Neuropathy and Its Symptoms
Diabetic neuropathy is a common complication of diabetes type 2:
- Types of Diabetic Neuropathy:
- Peripheral neuropathy (most common)
- Autonomic neuropathy
- Focal neuropathy
- Proximal neuropathy
- Symptoms of Peripheral Neuropathy:
- Numbness or reduced sensation in the feet and legs
- Tingling or burning sensations
- Sharp pains or cramps
- Increased sensitivity to touch
- Muscle weakness
- Loss of reflexes, especially at the ankle
- Foot deformities
- Symptoms of Autonomic Neuropathy:
- Bladder problems (incontinence or retention)
- Digestive issues (constipation, diarrhea, nausea)
- Sexual dysfunction
- Difficulty recognizing hypoglycemia (due to impaired adrenaline response)
- Abnormal heart rate and blood pressure control
- Diagnosis:
- Physical examination (checking reflexes, sensation, and muscle strength)
- Nerve conduction studies
- Electromyography (EMG)
- Quantitative sensory testing
- Management:
- Tight glucose control
- Pain management (medications like gabapentin or pregabalin)
- Regular foot care and inspections
- Treatment of specific symptoms (e.g., medications for digestive issues)
Understanding the Risks of Long-term Hyperglycemia
Long-term hyperglycemia can lead to various complications:
- Cardiovascular Disease:
- Increased risk of heart attack and stroke
- Development of coronary artery disease
- Peripheral artery disease
- Kidney Disease (Diabetic Nephropathy):
- Gradual loss of kidney function
- May lead to end-stage renal disease requiring dialysis or transplant
- Eye Problems (Diabetic Retinopathy):
- Damage to blood vessels in the retina
- Can lead to vision loss or blindness if untreated
- Foot Problems:
- Increased risk of infections
- Poor wound healing
- In severe cases, may lead to amputation
- Skin Conditions:
- Increased susceptibility to bacterial and fungal infections
- Development of diabetic dermopathy
- Cognitive Impairment:
- Increased risk of dementia and Alzheimer’s disease
- Dental Problems:
- Higher risk of gum disease and tooth decay
Monitoring for Other Complications: A Comprehensive Approach
A comprehensive approach to monitoring diabetes complications includes:
- Regular Eye Exams:
- Annual dilated eye exams to check for retinopathy
- Kidney Function Tests:
- Annual urine albumin test and estimated glomerular filtration rate (eGFR)
- Cardiovascular Assessments:
- Regular blood pressure checks
- Lipid panel tests
- Electrocardiogram (ECG) as needed
- Foot Examinations:
- Regular foot checks during office visits
- Annual comprehensive foot exam
- Dental Check-ups:
- Regular dental exams and cleanings
- Skin Inspections:
- Regular skin checks for infections or abnormalities
- Neurological Assessments:
- Periodic checks for neuropathy symptoms
- Mental Health Screening:
- Assessment for depression and diabetes distress
- Immunizations:
- Ensuring patients are up-to-date on recommended vaccinations
- Laboratory Tests:
- Regular monitoring of HbA1c, fasting glucose, and other relevant markers
Related Article
FAQs
How do you explain diabetes type 2 to a patient?
Type 2 diabetes is a chronic condition where your body either doesn’t produce enough insulin or has become resistant to its effects. This leads to high blood sugar levels, which can cause various health problems over time. It’s often related to lifestyle factors and can be managed through diet, exercise, and sometimes medication.
What is the best description of type 2 diabetes?
Type 2 diabetes is a metabolic disorder characterized by high blood sugar levels resulting from the body’s ineffective use of insulin. It’s the most common form of diabetes, often developing in adults and associated with obesity and sedentary lifestyle.
What is the clinical presentation of diabetes mellitus type 2?
The clinical presentation of type 2 diabetes can include increased thirst, frequent urination, unexplained weight loss, fatigue, blurred vision, slow-healing wounds, and recurrent infections. However, some patients may be asymptomatic and diagnosed through routine blood tests.
What is diabetes type 2 concept?
The diabetes type 2 concept refers to the understanding that this form of diabetes is primarily characterized by insulin resistance and relative insulin deficiency. Unlike type 1 diabetes, where the pancreas doesn’t produce insulin, in type 2 diabetes, the body becomes less responsive to insulin or doesn’t produce enough to maintain normal blood glucose levels.